
Blog & News





SHADAC Responds to Proposed American Community Survey (ACS) Sexual Orientation and Gender Identity (SOGI) Test Questions
December 4, 2023:|
View the U.S. Census Bureau's full request for comments in the September 19th edition of the Federal Register. |
On September 19, 2023, the U.S. Census Bureau released a request for comments regarding the proposed addition of test questions regarding sexual orientation and gender identity (SOGI) for the American Community Survey (ACS). According to the notice in the Federal Register, the Census Bureau specifically hopes to test question wording, response categories, and placement within the survey itself.
Researchers at SHADAC reviewed the proposed test questions included in the Register proposal, as well as the methodology and reasoning behind the Census Bureau’s choices, and responded with comments regarding the measurement of sex and gender identity. Specifically, researchers discuss the limitations of the two-step gender identity questions, language and inclusivity concerns, and recommendations for a more streamlined and accessible two-step question format.
SHADAC’s Comments on Measuring Sex and Gender Identity
When designing survey questions, the consumer experience is paramount. Maximizing the accessibility and acceptability of question language improves data quality in multiple dimensions, including item non-response, misclassifications, and overall response rates.
In the case of measuring sex and gender identity, context matters. It is important to acknowledge how these questions might differ in various settings - when asked on a survey compared to when asked in an administrative or clinical setting, for example. We are concerned that the ACS is missing a key opportunity to update questions on sex and gender in ways that both enhance user experience and are specific to the survey setting.
The test questions for sex and gender identity as proposed use overly academic language that is better suited for a clinical setting, by asking first ‘what sex was NAME assigned at birth’ followed by ‘current gender identity.’ While such questions have utility, such as for verification of specific health insurance benefits, this approach is not optimal for a population survey such as the ACS.
Unnecessary jargon makes questions less accessible for respondents with lower literacy levels or who are non-English speaking and adds to the cognitive burden for all respondents. Survey language should minimize the respondent burden in order to support data quality and user experience. The limitations of the proposed two-step gender identity question have been described by the National Academies of Sciences, Engineering, and Medicine (NASEM).
Specific concerns worth highlighting are:
1) The proposed response options for ‘current gender’ are not inclusive of transgender experiences because these options imply that transgender is a tertiary or ‘other’ category and mutually exclusive from male or female identities. Allowing for multiple answers (one of the proposed test options) does not address this conceptual limitation.
2) Asking chronologically about ‘sex assigned at birth’ followed by ‘current gender identity’ may be perceived as invasive and/or invalidating for transgender respondents, which could increase item nonresponse for this critical population.
3) Asking a third question for verification of gender status when a respondent’s answers to ‘sex assigned at birth’ and ‘current gender’ don’t match places an undue burden on the transgender and nonbinary population. At minimum, the testing process should assess false positive rates and seek to avoid unnecessarily burdensome questioning of transgender and nonbinary people.
4) ‘Sex assigned at birth’ is not inclusive of intersex or nonbinary designations on infant birth certificates. These situations are increasingly common, and the current wording could lead to false positives for transgender, along with unnecessarily invasive questioning among individuals born with intersex traits.
SHADAC recommends that the Census consider a more streamlined two-step question approach that gathers the same information (sex assigned at birth and current gender) while providing a more inclusive and accessible experience for respondents. Specifically, we recommend asking first ‘what is your gender’ followed by ‘are you transgender.’ This approach was developed in Oregon via extensive stakeholder engagement. Similar language has also been used by administrators to update population survey questions in Minnesota.
The alternative two-step question addresses the limitations described above in the following ways:
1) Response options for ‘gender’ should include male, female, nonbinary, and a write-in response option. Asking about transgender identity in a separate question avoids portraying transgender as mutually exclusive with male or female. For respondents who need an explanation for ‘transgender,’ a hover box or an interviewer can provide a definition as follows: ‘Transgender describes a person whose gender identity differs from their sex assigned at birth.’
2) Asking simply about ‘gender’ first is clear and inclusive. Avoiding the ‘sex assigned at birth’ initial question would be less duplicative and more accessible for many respondents.
3) Asking directly about transgender identity (with ‘yes/no’ response options) prioritizes accessible language to minimize respondent burden and may eliminate the need for additional verification for transgender respondents. Ethically, the ACS should avoid asking all transgender respondents for extra verification without strong data to indicate that doing otherwise would lead to significantly elevated false positive rates.
4) Not asking about ‘sex assigned at birth’ avoids unnecessary collection of personal health data. This supports privacy for all respondents. Additionally, this approach could help reduce item nonresponse and false positives among intersex individuals as well as cisgender respondents who are unfamiliar with and/or dislike the language and concepts in the initially proposed test questions.
Thank you for your consideration. We know that the Census Bureau faces many important decisions and appreciate the chance to share our feedback on this important content test.
Blog & News

2022 ACS Tables: State and County Uninsured Rates, with Comparison Year 2021
November 17, 2023:Each year, SHADAC uses data released from the American Community Survey (ACS) via the U.S. Census Bureau's data.census.gov tool to produce estimates of uninsurance at the state and county level.*
Click on a state below in the interactive map to see a PDF table of uninsured rates by state and sub-state geographies, but also by demographic characteristics (e.g., age, race/ethnicity, and poverty level) for 2022 and comparison year 2021.
Click here to view uninsurance estimates for the United States.
Click here to view uninsurance estimates for Puerto Rico and its municipios.
Note: These tables present uninsured rates, which indicate the share of the population that is uninsured. For example, a 10 percent uninsured rate for adult women indicates that 10 percent of all adult women are uninsured.
Maps & Tables of Private, Public, & Uninsured Changes from 2021 to 2022
- Private Coverage Rates by State, Change from 2021 to 2022, for All People
- Public Coverage Rates by State, Change from 2021 to 2022, for All People
- Uninsurance Rates by State, Change from 2021 to 2022, for All People
About the ACS
The ACS is a household survey that began in 2005 and produces annually updated data on a variety of population characteristics, including health insurance coverage. In total, the ACS surveys approximately three million U.S. households each year. An important feature of the ACS is that it includes a large enough sample for state‐level and sub‐state estimates.
The ACS began asking survey respondents about health insurance coverage during the 2008 calendar year. Specifically, the survey asks respondents about current coverage for each person in the respondent’s household. A person is categorized as “insured” if he or she has coverage at the point in time at which the survey is administered.
*Why Aren’t Estimates Provided for All Counties?
Due to sample size constraints, single-year ACS estimates are available at the county level only for counties with a population greater than 65,000.
How Are These Estimates Different from the Estimates that SHADAC Publishes Using Census Bureau Micro-Data Files?
Two definitions used by the Census Bureau to generate the tabulations above differ from those that SHADAC uses to generate tabulations for State Health Compare. The definitional differences are as follows:
Family
The Census Bureau defines a family as “all related people in a household.”
SHADAC defines a family using a measure called the “Health Insurance Unit” (HIU), which includes all individuals who would likely be considered a family unit in determining eligibility for either private or public coverage.
To learn more about the 2020 update of SHADAC's Health Insurance Unit (HIU) see our HIU resource page, which houses two issue briefs: The first describes the SHADAC HIU, its purpose, the most recent update, and improvements to HIU data inputs; and the second outlines the impacts of using the SHADAC HIU in analysis so that researchers can assess whether the SHADAC HIU is suitable for their research and what the potential impacts of its use might be. The page also provides a link to STATA and SAS codes to aid in the use of the HIU variable.
Family Income
The Census Bureau determines family income as a percentage of the Federal Poverty Level (FPL), which is a definition of poverty used primarily for statistical purposes. For example, FPL is used to estimate the number of Americans living in poverty each year.
SHADAC determines family income as a percentage of the U.S. Department of Health and Human Services’ Federal Poverty Guidelines (FPG), which is a measure used for administrative purposes. For example, FPG is used to determine eligibility for federal programs such as Medicaid and the Supplemental Nutrition Assistance Program (SNAP).
To learn more about the difference between FPL and FPG, read our updated blog post from April 2023.
Related ACS Materials:
- An Annual Conversation with the U.S. Census Bureau: 2022 Health Insurance Coverage Estimates from the ACS and CPS
- 2022 ACS: Declining Uninsured Rates for the U.S. and States are Supported by Private and Public Coverage Increases
- CPS ASEC: 2022 National Health Insurance Coverage Estimates Show Falling Rates of Uninsurance and Direct-Purchase Coverage (Infographic)
Publication
An Annual Conversation with the U.S. Census Bureau: 2022 Health Insurance Coverage Estimates from the ACS and CPS
On Thursday, September 28th at 1:00 PM CST, SHADAC hosted a webinar covering the release of new 2022 health insurance coverage estimates from two key, large-scale federal data sources: The American Community Survey (ACS) and the Current Population Survey (CPS).
Estimates from both surveys were presented at: the national and state levels, as well as by coverage type, and a range of other demographic categories (age, geography, poverty level, and more), during the webinar. Technical and analytic insight was provided from experts at the U.S. Census Bureau, which administers both the ACS and CPS, and SHADAC researchers joined with our special guests from the Census Bureau to answer questions from attendees after the presentation.
Attendees were able to learn about:
- New 2022 health insurance coverage estimates
- When to use which estimates from the ACS vs the CPS
- How to access the estimates via Census reports and the data.census.gov website
- How to access state-level estimates from the ACS using SHADAC tables and State Health Compare web tool
Speakers
 Kathleen T. Call, Moderator Kathleen T. Call, Moderator
Principal Investigator
SHADAC Dr. Call has been an Investigator with SHADAC since its launch in 2001. She is also a Professor in the Division of Health Policy and Management at the University of Minnesota (UMN), School of Public Health (SPH). She demonstrates her commitment to community-engaged scholarship through her leadership in the Clinical and Translational Science Institute, and the Interdisciplinary Research Leaders (IRL) program, and by co-chairing the UMN, SPH Health Equity Work Group.
|
 Katherine Keisler-Starkey, Speaker Katherine Keisler-Starkey, SpeakerEconomist in Health and Disability Statistics Branch United States Census Bureau Katherine Keisler-Starkey is an economist in the Health and Disability Statistics Branch in the U.S. Census Bureau’s Social, Economic and Housing Statistics Division. In her position, Ms. Starkey provides subject matter expertise on health topics for the Current Population Survey Annual Social and Economic Supplement (CPS ASEC) and has authored the Census Bureau’s Health Insurance Coverage in the United States report for the last four years. Her research interests focus on Applied Microeconomics, including Health Economics, Public Finance, and Labor Economics, and she is the author of several topically focused Census working papers and blogs in these areas. |
 Robert Hest, Speaker Robert Hest, SpeakerSenior Research Fellow
SHADAC Robert Hest joined SHADAC in 2017 and was recently made Senior Research Fellow. Mr. Hest provides expertise in survey data, data analysis and processing, and project management. Mr. Hest also manages SHADAC’s State Health Compare website, coordinating data processing, quality assurance, dissemination, and documentation of data.
|
 Sharon Stern, Speaker Sharon Stern, SpeakerAssistant Division Chief
United States Census Bureau Sharon Stern is the Assistant Division Chief for employment characteristics in the U.S. Census Bureau’s Social, Economic and Housing Statistics Division. In her position, Ms. Stern oversees statistics on the labor force, health insurance and disability from several Census Bureau surveys. She has authored a wide variety of Census Bureau reports and papers on topics related to poverty, disability, and health insurance.
|
Related Resources
SHADAC
- Webinar slides from SHADAC
- CPS ASEC: 2022 National Health Insurance Coverage Estimates Show Falling Rates of Uninsurance and Direct-Purchase Coverage (Infographic) (Blog)
- 2022 ACS: Declining Uninsured Rates for the U.S. and States are Supported by Private and Public Coverage Increases (Blog)
U.S. Census Bureau
- Webinar slides from Census Bureau
- Health Insurance Coverage in the United States: 2022 (Report)
- Health Insurance Coverage of U.S. Workers Increased in 2022: Health Insurance Rates for Working-Age Adults Higher by Race, Hispanic Origin, Region (Blog)
- Uninsured Rates Decreased in Over Half of U.S. States in 2022: Changes in Types of Health Insurance Coverage Contributed to Declines in Uninsured Rates From 2021 to 2022 (Blog)
Blog & News
Hest, Robert
Lanigan, Lindsey
Stewart, Andrea
2022 ACS: Declining Uninsured Rates for the U.S. and States are Supported by Private and Public Coverage Increases
Setember 14, 2023:
Related Releases and Materials
|
The U.S. Census Bureau released 2022 health insurance coverage estimates from the American Community Survey (ACS) today, which included state-level information about health insurance coverage by type as well by certain demographic categories. The Census Bureau also released an accompanying report and blog post highlighting many of the changes seen from 2021 to 2022.
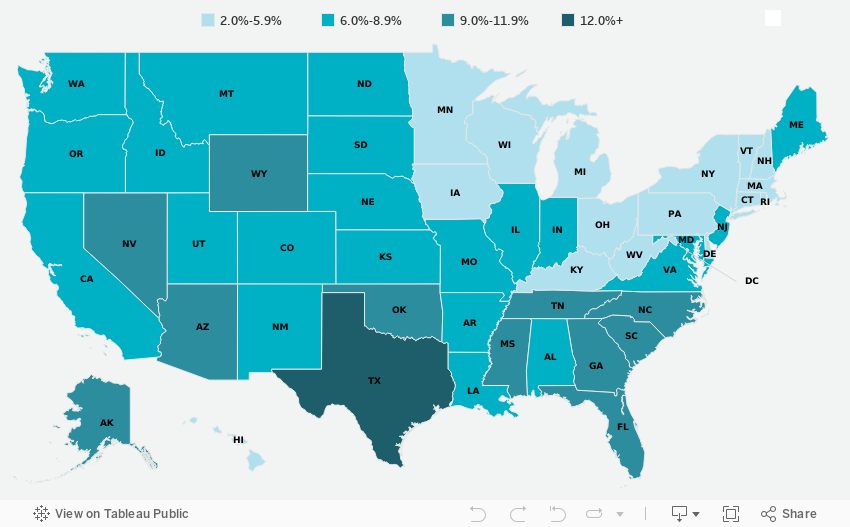
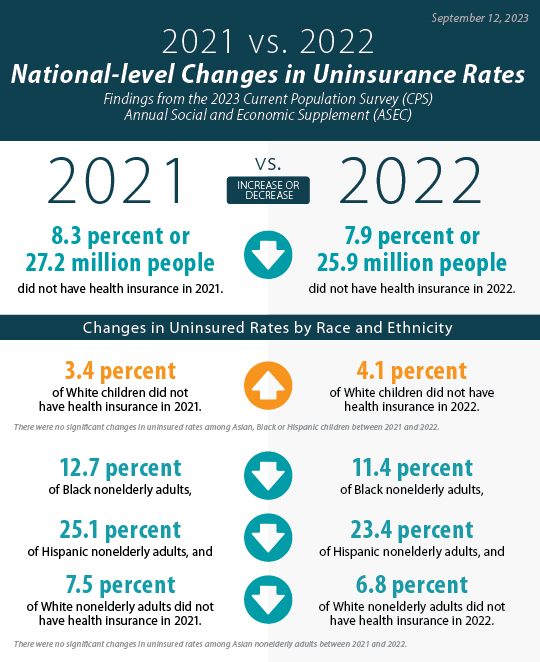
Overall, the data showed a drop in uninsured rates, with an 8.0% rate of uninsurance in 2022 as compared to 8.6% in 2021. This echoes similar year-over-year decreases in uninsurance shown in data from the Current Population Survey (CPS), for which estimates were released on Tuesday, and in recent survey data from the National Health Interview Survey (NHIS). Eight percent represents the lowest-ever national rate of uninsurance measured in the ACS.
The national decline in uninsurance was supported by decreases in 27 states, with Maine the only state to see an increase in its uninsured rate, from 5.7% in 2021 to 6.6% in 2022, reversing the previous trend from 2019 to 2021.* Overall, uninsured rates ranged across states from a low of 2.4% in Massachusetts to a high of 16.6% in Texas, a continuing trend from past years. The largest drop in uninsured rates was found in Oklahoma, which fell by 2.1 percentage points (PP) to 11.7% in 2022 from 13.8% in 2021.
The drop in uninsured rates coincided with small yet significant increases in 2022 for both private coverage — 67.2% from 67.0% in 2021 — and public coverage — 37.2% from 36.8%. Alaska saw the largest increase in private coverage, rising 2.2 PP to 66.4%. Nine states saw increases in private coverage, while nine states saw decreases in private coverage. And unsurprisingly, Oklahoma saw the largest increase in public coverage, rising 2.3 PP to 39.6%: Oklahoma was one of two states, along with Missouri to have expanded Medicaid in 2022.
The rest of this blog post highlights some of the national and state-level changes that took place between 2021 and 2022 in the broadest categories of insurance (uninsurance, public coverage, and private coverage) for two key age groups, nonelderly adults (age 19-64) and children (age 0-18). Accompanying interactive maps allow readers to view and sort the different coverage types for each age group.
Key Findings from the 2022 ACS: Nonelderly Adults (19-64)
Figure 1. Changes in state-level coverage rates among nonelderly adults, 2021-2022
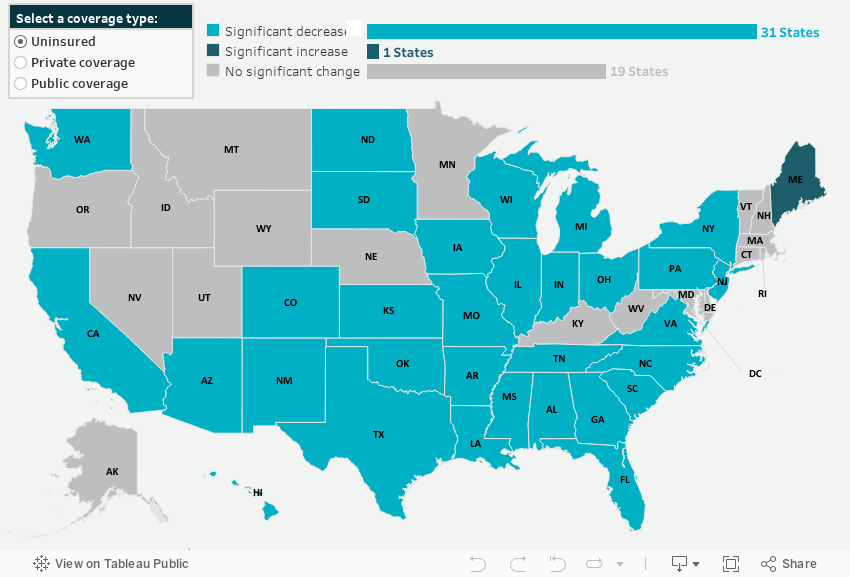
State-Level Uninsurance
Nonelderly adults also saw falling uninsurance rates, dropping by 0.9 PP from 12.2% in 2021 to 11.3% in 2022. Additionally, 31 states saw decreases in their uninsured rates for nonelderly adults while only Maine saw an increase, rising 1.4 PP to 9.6%. The largest decline in uninsurance was seen in Oklahoma, whose rate of uninsured nonelderly adults dropped a notable 3.4 PP to 16.8% in 2022.
State-Level Private Coverage
Private coverage increased significantly for nonelderly adults, rising 0.7 PP to 73.4% in 2022 from 72.7% in 2021. This increase was echoed across 21 states, with Mississippi seeing the largest increase at 2.2 PP, rising to 69.7% in 2022. Private coverage levels fell across just three states — Maine, Minnesota, and Virginia — with Maine seeing the most significant drop, falling 1.8 PP to 74.1% in 2022.
State-Level Public Coverage
Overall, nonelderly adults also experienced a significant increase in public coverage from 2021 to 2022. Rates of public coverage rose to 19.4% from 19.1% in 2021, driven by similar increases across 14 states. Individually, Oklahoma once again saw the largest increase — 19.9%, up from 16.3% in 2021. Of the eight states that saw decreases in 2022, public coverage for nonelderly adults declined the most in Rhode Island, dropping 2.1 PP to 21.7
Key Findings from the 2022 ACS: Children (0-18)
Figure 2. Changes in state-level coverage rates among children, 2021-2022
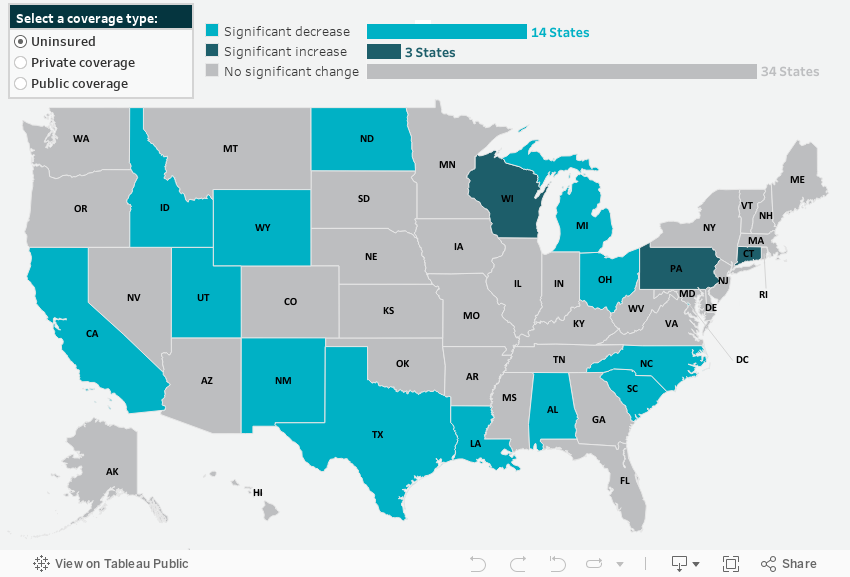
State-Level Uninsurance
For children, uninsured rates fell to 5.1% in 2022 from 5.4% in 2021. Fourteen states also saw drops in children’s uninsurance, Wyoming being the largest - falling 3.5 PP to 7.9%, followed by New Mexico, which saw a 2.6 PP decrease from 6.4% in 2021 to 3.8% in 2022. Three states (Connecticut, Pennsylvania, and Wisconsin) saw increased children’s uninsured rates for 2022.
State-Level Private Coverage
Unlike nonelderly adults, children did not experience an overall increase in private coverage for 2022. Private coverage remained statistically unchanged for children nationally at 60.6%. However, 13 states did see rising private coverage rates, with Rhode Island leading the way, jumping 4.8 PP to 69.4% in 2022. Six states saw declines in private coverage, led by a drop of 2.3 PP in Missouri, whose rate of private coverage for children in 2022 was 63.2%.
State-Level Public Coverage
Like private coverage rates, public coverage remained statistically unchanged for children from 2021 to 2022, sitting at 39.6%. Just eight states saw increased public coverage for kids in 2022, led by a 2.6 PP jump in North Dakota, from 21.3% in 2021 to 23.9% in 2022. And seven states saw declining public coverage rates, with children in Rhode Island experiencing a precipitous fall of 5.9 PP to 34.4% in 2022.
Future Data Releases and Products
Supplemental tables for the 2022 ACS 1-Year Estimates will be released from the U.S. Census Bureau on October 19, 2023, and 2018-2022 ACS 5-Year Estimates will be available on December 7, 2023.
Stay tuned for more granular details about insurance coverage changes in the states from 2021 to 2022 via customized SHADAC tables examining coverage at the state and county level, and for an announcement of updated health insurance coverage measures available on State Health Compare.
Notes
All changes described in this document are significant at the 90% level. Private coverage includes individually purchased, employer-sponsored coverage, and TRICARE military health coverage Public coverage includes Medicare, Medicaid/CHIP, and VA health care. Public and private coverage types are not exclusive and include individuals with those types of coverage alone or in combination with other coverage. Estimates represent the civilian noninstitutionalized population.
Overarching estimates of uninsurance and public and private coverage are for all ages, except where noted for children (age 0-18) and nonelderly adults (19-64).
COVID-19 Public Health Emergency Impacts
Continuous Coverage Requirement
The continuous coverage requirement that prevented states from terminating individuals’ Medicaid coverage during the pandemic ended on March 31, 2023. The resumption of Medicaid eligibility redeterminations and renewals (and potential disenrollments), a process commonly referred to as the “unwinding,” began on April 1, 2023, and each state has a year to navigate a return to normal operations while also meeting reporting requirements set by CMS for publicly sharing coverage transitions and outcomes data during this time. While the health insurance estimates released by the US Census Bureau for 2022 precede the beginning of the unwinding process, the data provide an essential baseline for understanding how health insurance coverage is distributed across the U.S. and among the states prior to the unwinding, as well as marker to measure the impacts of this seismic coverage transition as potentially millions of individuals, both adults and children, are poised to lose Medicaid and must either find another form of coverage (e.g., state-based marketplace or employer-sponsored insurance [ESI]), or risk becoming uninsured.
Several resources have been compiled by SHADAC to track the unwinding process in a variety of avenues, falling under several broader categories:
Guidance for States
- Using Surveys to Monitor Coverage Transitions During the Unwinding of the Medicaid Continuous Coverage Requirement
- Best Practices for Publicly Reporting State Unwinding Data
Health Insurance Coverage Data Tracking
- State-Based Marketplace Transition Data During the Unwinding
- State Dashboards to Monitor the Unwinding of the Medicaid Continuous Coverage Requirement
- Tracking Health Insurance Coverage During the Unwinding: Monthly Data from the Household Pulse Survey
*Data Collection and Dissemination
As has been extensively documented by both SHADAC and the Census Bureau, disruptions to data collection and dissemination efforts—as well as the presence of significant nonresponse bias—due to the COVID-19 pandemic heavily impacted estimates for 2020. As such, the Census Bureau released 2020 ACS 1-year data in an “experimental-only” format and cautioned against their use. Similarly, the Census Bureau recommends that data users do not compare 2020 ACS 1-year experimental estimates with any other data. Researchers therefore have compared 2019 to 2021 data.
Blog & News
Hest, Emily
Hest, Robert
Community and Uninsured Profile In Action: Local Case Studies
June 8, 2023:With the recent end of the public health emergency and subsequent “unwinding” of the Medicaid continuous coverage requirement, many Americans are now having to navigate changes in health insurance coverage. And while coverage transitions aren’t unique to this moment, the unwinding has spurred many states to think critically about how to mitigate the impacts of this event on potentially vulnerable populations.
Existing data on local communities is invaluable for states considering their approach for helping their residents secure coverage both now and beyond this historic moment. The Minnesota Community and Uninsured Profile is one example of the type of data that can make a meaningful difference in efforts to reach and cover communities. The Minnesota Community and Uninsured Profile features population details and characteristics that can be applied for a variety of different purposes; below are two case studies highlighting how the profile can support the enrollment efforts of local organizations and departments.
Community and Uninsured Profile in Action
Open Door Health Center Case Study
Open Door Health Center (ODHC) is a community health center that serves southern Minnesota. Given that ODHC serves a broad geographic area with limited staffing and resources, the team has to be strategic about how they do community outreach and enrollment. The profile helps ODHC identify specific areas in southern Minnesota with concentrations of uninsured individuals who are potentially disconnected from health care resources. Their navigators can then conduct enrollment and educational events within those areas, equipped with the important context on the local population found in the profile.
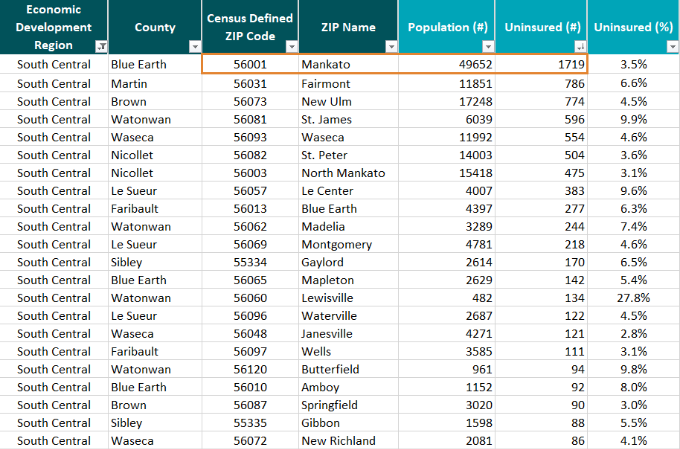 Staff at ODHC used the “ZIP Code Uninsured Rates” tab in the profile to hone in on the 24 community ZIP Codes in their region (South Central, MN) with available data. Among those communities, Mankato (56001) has the largest number of uninsured at 1,719 people which could make it a logical site for enrollment and outreach efforts.
Staff at ODHC used the “ZIP Code Uninsured Rates” tab in the profile to hone in on the 24 community ZIP Codes in their region (South Central, MN) with available data. Among those communities, Mankato (56001) has the largest number of uninsured at 1,719 people which could make it a logical site for enrollment and outreach efforts.
By entering “56001” in the Uninsured Profile tab, they could get more pertinent information about Mankato to help effectively target outreach. For example, they would see that among the uninsured in this community:
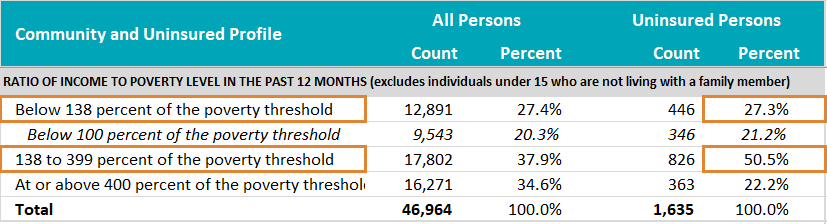 More than a quarter are likely income eligible for Minnesota Medical Assistance (<138% of the federal poverty level [FPL]) and more than half are likely income eligible for subsidized coverage through MNsure (138-400% FPL)
More than a quarter are likely income eligible for Minnesota Medical Assistance (<138% of the federal poverty level [FPL]) and more than half are likely income eligible for subsidized coverage through MNsure (138-400% FPL)
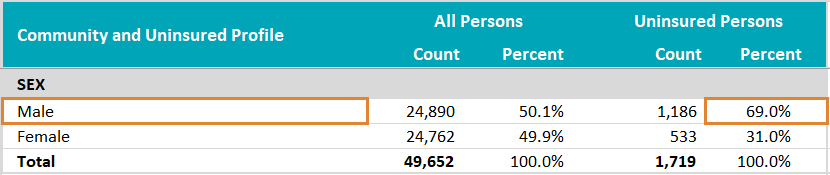 Nearly 70% are male;
Nearly 70% are male;
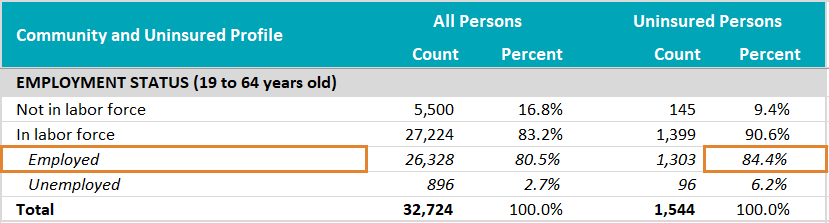 More than 80% are currently employed;
More than 80% are currently employed;
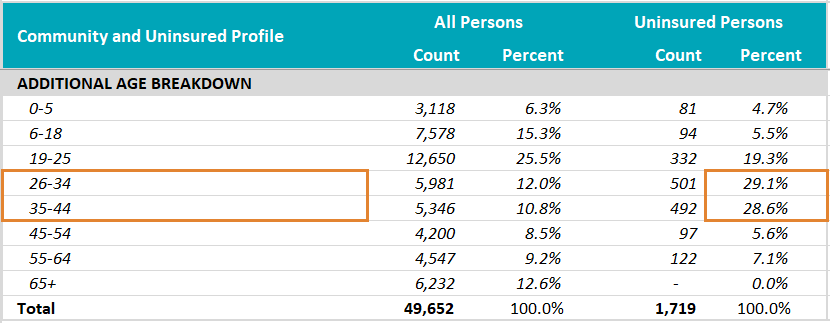 And nearly 60% are between the ages of 26 and 44.
And nearly 60% are between the ages of 26 and 44.
Based on these characteristics, staff at ODHC could set up enrollment events in partnership with employers of low-wage workers, or target outreach with messages and venues that speak to male residents or adults in early to middle age. ODHC could be confident that many of the uninsured community members they reach would be income-eligible for some type of free or subsidized coverage.
Further, looking at the profile, ODHC staff could observe that though there are a relatively small number of uninsured Hispanic/Latino residents of this community (211 persons), that group has a high uninsured rate (10.1%), especially compared to Mankato’s comparatively low community uninsured rate of 3.5%. This could indicate that further work needs to be done specifically to cover the Hispanic and Latino residents of Mankato.
Nicollet County Case Study
Nicollet County's local public health department serves a population of about 33,000. Like ODHC, they use the profile to review the demographics of those who are uninsured in their community to inform outreach efforts. The Community and Uninsured Profile also helps them target influenza and COVID-19 vaccinations for underinsured and uninsured community members. The department also uses the profile to better understand the characteristics of individuals who are uninsured in their communities through demographic filters such as race and ethnicity.
Looking in the ZIP Code Uninsured Rates tab, there are two ZIP-Code-defined communities (with available data) in Nicollet County: St. Peter (56082) and North Mankato (56003). Both have relatively low uninsured rates at 3.6% and 3.1%, respectively, and both have around 500 uninsured residents.

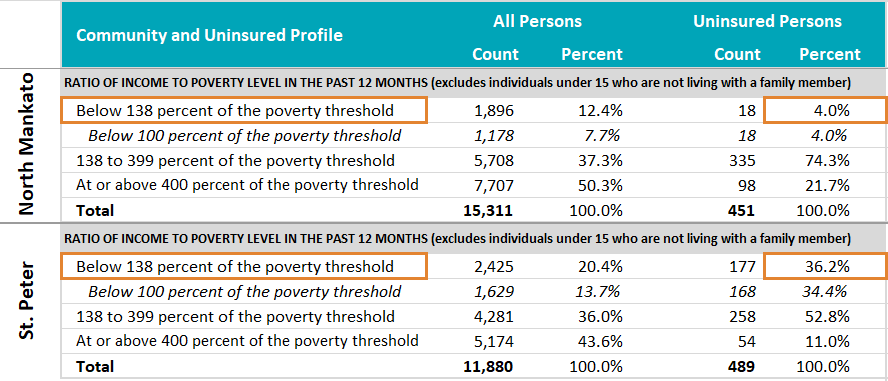 However, there are important differences between these communities that are evident when looking in the Uninsured Profile tab. For example, though less than 5% of the uninsured in North Mankato appear to be income-eligible for Medical Assistance (<138% FPL), more than 36% of the uninsured in St. Peter appear to be income-eligible for that program.
However, there are important differences between these communities that are evident when looking in the Uninsured Profile tab. For example, though less than 5% of the uninsured in North Mankato appear to be income-eligible for Medical Assistance (<138% FPL), more than 36% of the uninsured in St. Peter appear to be income-eligible for that program.
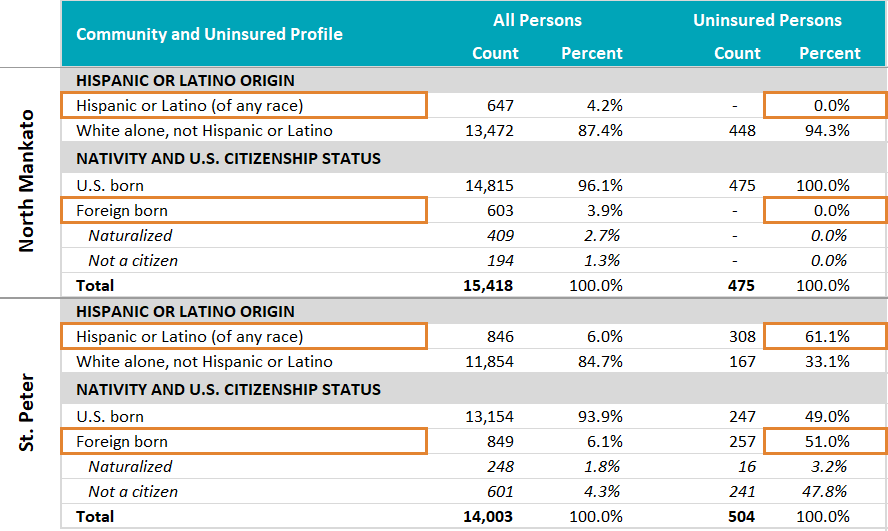
Further, whereas none of the uninsured in North Mankato are Hispanic or Latino, Hispanic or Latino residents make up more than 60% of the uninsured in St. Peter. And there is a similar story by citizenship status and nativity; whereas all of North Mankato’s uninsured are U.S. born, more than 50% of St. Peter’s uninsured are foreign born, and more than 90% of those are not citizens, which creates policy and financial barriers to accessing insurance and health care.
The different characteristics of the uninsured in these two communities call for different strategies for outreach and enrollment efforts, such as providing culturally appropriate materials, selecting different sites or partners for enrollment events, and being prepared to enroll uninsured community members into different types of health coverage programs.
What are your Community and Uninsured Profile stories?
Are you a part of an organization that uses the Minnesota Community and Uninsured Profile? We would love to hear stories of how you have used the profile in your work. If you have a story to share, please send it to shadac@umn.edu.

