
Blog & News





Considerations from SHADAC: Proposed Revisions to Federal Standards for Collecting Race/Ethnicity Data
March 23, 2023:
|
On January 26, 2023, the Interagency Technical Working Group on Race and Ethnicity Standards released an initial set of recommended revisions to the Office of Management and Budget’s (OMB) Statistical Policy Directive No. 15: Standards for Maintaining, Collecting, and Presenting Federal Data on Race and Ethnicity (SPD 15). SHADAC summarized the proposed revisions to the OMB standards in a recent State Health & Value Strategies Expert Perspective. The public was invited to provide comment on the proposed revisions, and below, we provide text from the feedback that SHADAC submitted to Dr. Karin Orvis, Chief Statistician of the United States, in response to these revisions. We encourage other interested parties to also submit their comments, especially those who can provide state-level perspectives such as state data analysts and policymakers. |
Response from SHADAC
The State Health Access Data Assistance Center (SHADAC) is a health policy research center within the University of Minnesota School of Public Health. We provide technical assistance (TA) to states in the areas of data use and analysis to support policy. The below comments are based on SHADAC’s specific experience supporting states as they address challenges related to the collection of data on race, ethnicity, language, disability, sexual orientation, and gender identity via the Medicaid application.
SHADAC was thrilled to see the revised OMB standards related to the collection of race and ethnicity. The proposed revisions align with available evidence, are consistent with the changes made by leading states, and most importantly, explicitly state that these standards should serve as a minimum baseline with a call to collect and provide more granular data. However, while these standards are specifically named as minimum reporting categories for data collection throughout the Federal Government, if adopted, they are likely to shape data collection and reporting across all sectors, including the states with whom we work that collect race/ethnicity data through the Medicaid application process.
State Medicaid programs have the flexibility to develop their own applications and race and ethnicity questions as long as they meet CMS-established reporting requirements (which follow current OMB guidance). Although many states follow the application model that CMS developed in 2013, our research has found 65 different variations in how these data are collected across all states and modes (e.g., paper, online). Once collected, this information is used in a wide variety of ways: to support state analysis and operation; in reporting to CMS; and to feed into the T-MSIS, which in turn is released as the research-ready T-MSIS data files used by researchers studying Medicaid program health outcomes, health equity, and administrative accountability.
Given the role OMB standards play in shaping state data collection approaches and the obvious impact and reach of these data, we respectfully submit our comments aimed at supporting the adoption of a revised set of standards.
Cross Program and Agency Alignment
Guidance needs to include detail on how any revisions will filter through data collection and reporting across all sectors that impact states/federal interactions. Will all federal agencies adopt the proposed new standards on the same timeline?
For example, all Food and Nutrition Services (FNS) state agencies are currently required to collect race and ethnicity according to prescribed specifications: race and ethnicity must be collected using a two-question format (ethnicity must be collected before race), and the minimum categories must align with OMB standards. Therefore, states with a combined Medicaid/SNAP application currently cannot offer a combined race/ethnicity question even though the most current evidence shows that is the preferred approach. States will want to know whether the adoption of the new proposed OMB standard allowing for a combined race/ethnicity question will supersede the existing FNS guidance on how to collect this information. Or will states that want to pursue a combined question on their combined Medicaid/SNAP application have to wait for updated FNS guidance to be released?
Similarly, existing guidance requires states to share data (including demographic data like race and ethnicity) with health plan carriers via a federally standardized 834 template. States cannot make changes to existing data fields on this form—any changes made currently result in enrollment transaction failures. If OMB standards are updated, how and when will changes be made to the 834 file form to align with these new changes?
Finally, the revisions have implications for state data reporting of race and ethnicity into the Transformed Medicaid Statistical Information System (T-MSIS). If approved, states will need guidance on how to transition to a single data element (combined race and ethnicity). They will need to understand how to streamline or roll-up more granular data and more write-in data and how to manage the likely increase in people who report more than one race.
Data Granularity
The revised guidance rightfully acknowledges the challenges associated with collecting more granular data. If the final guidance recommends the inclusion of an open text response option for each detailed category, states will need detailed, individual guidance on how best to manage those data. While most states prioritize granularity, they simply don’t have the staff time or, in some cases, the expertise to develop the thoughtful and detailed cleaning and coding procedures required to process a large volume of write-in data. In addition, many current IT systems don’t have the functionality to collect and store a large volume of write-in data.
One way to support this would be to develop or enhance an existing hierarchy that includes a long and diverse list of racial and ethnic categories, such as the Centers for Disease Control Race Category and Ethnicity Groupings. Another way to support the use and reporting of disaggregated data is to provide technical support and guidance around data use standards. This could include standards around recency, maximum “refusal to answer” thresholds, data missingness thresholds, and sample size thresholds that guide suppression of publication.
Technical Assistance
States need direct technical assistance (TA) to support the successful implementation of revised standards. This will need to go beyond documentation and guidance. To do this well, states should have access to experts who can provide practical, hands-on advice that is responsive to their specific needs. The type of assistance needed will vary. States with sophisticated analytic teams may seek advice on how to bridge race and ethnicity data collected under one method with data collected under a revised method. Other states may need more fundamental support to implement the expanded race/ethnicity option in a way that is the least disruptive to their current data collection structure.
We would also recommend that any TA effort include a forum for states to discuss implementation challenges with their peers and serve as a repository for promising practices. States will face different challenges but always appreciate having a forum to discuss problems and solutions with other state officials. In addition, there is limited research on best ways to collect data on race and ethnicity and even less on operational considerations for collecting this information in an administrative context like a Medicaid application. Technical assistance should encourage and support the evaluation of systems’ improvements and serve as a clearinghouse for sharing key findings.
To build trust with the enrollees from whom this data is being collected, states would also benefit from technical assistance or model training materials on the best ways to communicate why this data is being collected and how it is being used (e.g., TA on effective forms of community engagement, Navigator or assister training, or instructional language scripts for frontline workers.)
Funding
Questions that collect race and ethnicity data within the Medicaid application are embedded in many other complex and multifaceted questions about topics such as employment, income, household composition, etc. The systems that collect and house this information vary in their age, technical capacity, and purpose. Almost uniformly, they are complex and expensive to change, both in terms of data collection but also data transfer, reporting, and sharing. Ideally, states can access new dedicated funding or receive clear guidance on how existing federal money can be used to make necessary IT and systems changes.
The funding associated with this effort should also be flexible. It should support direct costs like system modifications but also priorities such as stakeholder engagement, instructional language development, and training—all of which are critical to successfully implementing the revised data collection guidance.
Urgency of Additional Guidance
While we are encouraged to see revised standards related to race and ethnicity data collection, we want to stress the urgency of revised guidance related to data collection on sexual orientation, gender identity, primary language, and disability. The current standards on sex are woefully inadequate, to the point of causing harm to people who identify as belonging to a sexual or gender minority population. Standards around disability and language are similarly lacking. Given the intersectionality of these concepts as they relate to identity, it’s important to make progress on updating standards for all areas, not just one. In addition, if states are to make significant investments to modify application wording as well as data systems and reporting structures to improve the collation of race and ethnicity, it makes sense to do this with the knowledge and understanding of timing for future changes regarding sexual orientation, gender identity, primary language, and disability. At the best, these timelines could be aligned, and at the least, states should have visibility to when those revisions are likely to be released.
Blog & News

Review of Health Insurance Coverage Data in 2021: Releases and Resources
February 27, 2023:Each year, SHADAC covers the releases of health insurance coverage data from major federal surveys such as the American Community Survey (ACS) and Current Population Survey (CPS), both of which are overseen by the U.S. Census Bureau.1 Not only do these data provide an understanding of trends for the millions of individuals in the United States who lack any type of coverage, but they also give indications of changes in other major forms of health insurance, like public coverage, private coverage, and employer-sponsored coverage.
SHADAC researchers work to provide insights into these data in a variety of formats (including reports, blog posts, and webinars) and analyze a multitude of important demographic groups (children, families living below poverty levels, and for communities of color). We also know that to truly understand the trends and vagaries of health insurance coverage, it’s important to look beyond national-level statistics, to see what’s happening at the state level.
That’s why we recently updated one of the longest-running measures on SHADAC’s data tool, State Health Compare, “Health Insurance Coverage Type” with the latest data for 2021. Users can take a look at estimates of health insurance coverage across all 50 states by type (uninsured, employer-sponsored, Medicaid/CHIP, etc.), by categories (age, education level, race/ethnicity, marital status, poverty level, etc.),2 over time (from 2008-2021),3 and can even examine estimates using color-coded maps, trend and bar charts, or by ranking states in terms highest and lowest rates for any coverage type.
2021 Key Findings
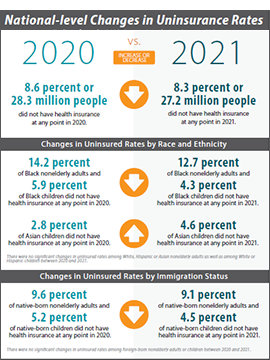
After multiple disruptions to data collection efforts resulted in data quality issues for 2020 ACS estimates, SHADAC is excited that data for 2021 are able to be used with confidence once again—though users are cautioned not to compare data to the prior year. Nationally, the U.S. saw a near-record low rate of uninsurance in 2021, at 8.6%, second only to a rate of 8.5% in 2016.
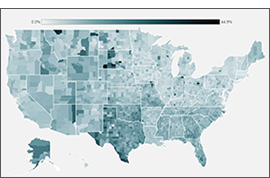
Looking at the state level, however, shows much wider variation in uninsured rates, from a low of 2.4% in Massachusetts to a high of 17.9% in Texas. By larger demographic groups:
- Among children (age 0-18), 5.4% were uninsured in 2021; however, by state, this ranged from 1.1% in Massachusetts to 11.8% in Texas.
- Among those below the poverty level, 15.6% were uninsured in 2021; however, by state, this ranged from 4.4% in Vermont to 30.5% in Texas.
- Among individuals with less than a high school degree, 22.2% were uninsured in 2021; however, by state, this ranged from 5.9% in Massachusetts to 41.4% in Texas.
- Among people reporting “Fair” or “Poor” health status, 25.9% were uninsured in 2021; however, by state, this ranged from 17.9% in Louisiana to 44.7% in Utah.
SHADAC Publications
For a full range of available products from SHADAC’s coverage of the 2022 health insurance data release (2021 estimates) please see below.
|
2021 CPS ASEC: National-level |
An Annual Conversation with |
Comparing Federal Government |
|
2021 ACS: State-level Analysis |
2019 vs 2021 ACS: State and |
2017-2021 ACS: 5-year State and |

- CPS ASEC: 2021 National Health Insurance Coverage Estimates Show Falling Uninsured and Private Coverage Rates Across Population Demographics (Blog & Infographic)
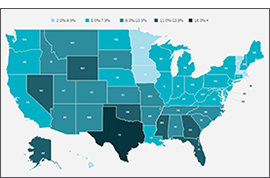
- 2021 ACS: Estimates Show Declining Uninsurance Rates Across 28 States, Driven by Rise in Public Coverage and Fall in Private Coverage (Blog & Interactive Maps)
- An Annual Conversation with the U.S. Census Bureau: Coverage Estimates from the 2021 ACS and CPS (Webinar Recording)
- 2021 ACS Data: State and County Uninsured Rates, with Comparison Year 2019 (Blog, Interactive Map, & Data Tables)
- Comparing Federal Government Surveys That Count the Uninsured: 2022 (Issue Brief)
- 2017-2021 ACS: 5-year Combined State and County Uninsured Rates (Blog, Interactive Map, & Data Tables)
For more detailed estimates on health insurance coverage in 2021, please visit State Health Compare. Be sure to also check out our helpful guide to Navigating Data on State Health Compare for more on what users can do with this unique data tool!
1 SHADAC also covers health insurance coverage data releases from both the National Health Interview Survey (NHIS) and the Medical Expenditure Panel Survey (MEPS). For more on the NHIS, see a recent blog post discussing the early release estimates from the first half of 2022, and for more on the MEPS, see the latest edition of our of Employer-Sponsored Health Insurance report.
2 Because of changes made in 2020 to how the ACS measures race and ethnicity, caution should be used when comparing data by race and ethnicity from 2021 and later to data from 2019 and earlier.
3 As previously documented by SHADAC, 2020 ACS data were unfortunately severely disrupted by the COVID-19 pandemic, resulting in the choice by the U.S. Census Bureau to release the estimates in an “experimental-only” capacity. For that reason, SHADAC created a special “Health Insurance Coverage Type (2020)” measure using data from the CPS. For more on the reasoning behind using the CPS instead of the ACS and the differences between the two surveys, please see our explanatory blog post.
Blog & News

Changing Population Estimates: Implications for Data Users
February 21, 2022:.
|
How the CDC’s recent shift will impact calculations for birth and death rates |
The National Center for Health Statistics (NCHS) at the Centers for Disease Control (CDC) recently changed the population estimates they use to calculate population-level rates in their National Vital Statistics System (NVSS), such as birth rates and mortality rates that are commonly accessed through tools such as CDC WONDER. These population estimates allow for the production of rates by providing a population denominator against which to compare the number of births or deaths.
Beginning with the 2021 data year, CDC transitioned from using "bridged-race" population estimates based on the race and ethnicity categories specified in the 1977 OMB Race and Ethnic Standards for Federal Statistics and Administrative Reporting to using "single-race" population estimates from the U.S. Census Bureau (“Census”) based on the race and Hispanic ethnicity categories specified in the 1997 OMB standards for the collection of data on race and ethnicity. The bridged-race estimates had been created to better align the population estimates from Census that used the 1997 OMB categories with the birth and death records from vital statistics systems that in many cases still used the 1977 OMB categories. This transition to the single-race population estimates appears to be precipitated by Census' recent improvement to their collection of race and ethnicity data beginning with Census 2020 data collection and continuing with subsequent years of the American Community Survey.
This move to single-race population estimates has several implications for data users:
- Statistics based on the single-race population estimates are only made available via CDC WONDER for data years 2018 forward, and statistics based on bridged-race population estimates are only available through data year 2020. Data users should not make comparisons between statistics based on bridged-race population estimates and statistics based on single-race population estimates. Further, because of changes made in 2020 to how Census measures race and ethnicity, caution should be used when comparing statistics by race and ethnicity from 2020 and later to data from 2019 and earlier.
- CDC WONDER has expanded the number of race and ethnicity categories available to data users. Previously, only five race categories and two Hispanic ethnicity categories were available. This has been expanded to up to 31 race categories and two Hispanic ethnicity categories.
- The single-race population estimates produced by Census suppress the number of persons less than five years of age at the county level to comply with Census' privacy policies. This prevents users from calculating age-adjusted rates at the county level or by level of urbanization using the single-race data, though crude rates can still be calculated at these levels of geography.
This change also affects SHADAC’s Suicide Deaths measure on State Health Compare. That measure’s Race and Ethnicity breakdown is now available in separate series for data years 1999–2020 and 2018–2021; estimates should not be compared between these series. Furthermore, SHADAC is unable to update the Metropolitan Status breakdown for this measure past data year 2020 due to the previously explained county-level suppressions.
Going forward, data users should keep changes in the denominator in mind when comparing annual estimates based on CDC vital statistics data. SHADAC strives to account for these types of considerations on State Health Compare by making clear when data years aren’t comparable and providing data users with relevant context around changes in methodology and data collection.
Blog & News
Recent Publication Round-Up: The 2021 Medicaid Undercount
February 1, 2023:Research has consistently shown that surveys that measure health insurance coverage underestimate the number of people enrolled in Medicaid; this is known as the “Medicaid undercount.” SHADAC researchers have long monitored and investigated the magnitude, causes, and effects of the Medicaid undercount across surveys such as the American Community Survey (ACS) and Current Population Survey Annual Social and Economic Supplement (CPS ASEC) and its prevalence across states and populations.
Two recent SHADAC publications investigate the large increase in the size of the undercount in the 2021 ACS, providing new information and guidance for data users:
The first, “Medicaid Undercount Doubles, Likely Tied to Enrollee Misreporting of Coverage,” describes the large increase in the undercount in the ACS, using longitudinal data from the CPS ASEC to analyze the extent to which the increase in the undercount may be tied to an increase in Medicaid enrollees’ misreporting of coverage due to the pandemic-era Medicaid continuous coverage requirement. |
The second, “Tracking the Medicaid Undercount in the 2021 ACS Coverage Data,” presents state variation in the 2021 ACS’ undercount, how analytic choices such as health insurance coverage hierarchies and misaligned analytic universes (i.e., all persons vs. noninstitutionalized persons) can affect the apparent size of the undercount, and best practices for using 2021 ACS coverage data in light of the increased undercount. |
SHADAC continues to monitor and investigate the Medicaid undercount in surveys of health insurance coverage. The undercount will remain an active area of interest as survey estimates of 2022 health insurance coverage are released later this year and as the “unwinding” of the Medicaid continuous coverage requirement begins this spring.
Publication
Tracking the Medicaid Undercount in the 2021 ACS Coverage Data
Research has consistently shown that health insurance coverage surveys underestimate the number of people enrolled in Medicaid and the extent of this “Medicaid undercount” varies greatly across surveys and states. Among these surveys that measure health insurance coverage, the American Community Survey (ACS) has been shown to have a smaller Medicaid undercount, which is one of the reasons that SHADAC typically relies on this survey to track state-level health insurance coverage.
The “Medicaid undercount” refers to the discrepancies that exist between survey estimates of enrollment in Medicaid and the number of enrollees that are actually reported in state and national administrative data.
With 2021 ACS data being given its normal, official release by the Census Bureau following COVID-19 pandemic-related disruptions, SHADAC is again using the ACS as our primary data source for monitoring state-level health insurance coverage. However, as we and other data users have begun analyzing the 2021 ACS data, it has become apparent that the extent of the ACS’ Medicaid undercount was larger in 2021 than in prior years.
Given the evidence of a greater Medicaid undercount in the 2021 ACS, it is important for users to understand the undercount in the ACS when interpreting coverage estimates. In this brief, we review the research regarding the Medicaid undercount in the ACS, provide estimates of how the undercount varies across states, discuss the impact of assigning single coverage for those with multiple sources on the Medicaid undercount in the ACS, and provide guidance on how to understand health insurance coverage data in the 2021 ACS.
Related SHADAC Resources
Medicaid Undercount Doubles, Likely Tied to Enrollee Misreporting of Coverage (Issue Brief)
Understanding the Undercount of Medicaid Enrollees in the 2020 CPS (SHADAC Blog)
Medicaid Expansion and the Medicaid Undercount in the ACS (Research Article)
Medicaid Undercount Project (Collaborative Study)

