
Publication



Minnesota LTSS Projection Model: MN-LPM

Blog & News

MACStats from MACPAC: 2018 Medicaid and CHIP Data Book Now Available
February 1, 2019: The Medicaid and CHIP Payment and Access Commission (MACPAC) recently released the 2018 version of its Medicaid and CHIP Data Book. This data book is a collection of federal and state statistics regarding the Medicaid and CHIP programs that are compiled by MACPAC from multiple data sources on key topic areas including Medicaid and CHIP eligibility, enrollment, and expenditures, as well as beneficiary health, service use, and access to care. An excellent resource, the data book draws on a wide variety of data sources including Medicaid administrative data (e.g., CMS-64 data, MSIS data, Medicaid Managed Care enrollment reports, etc.) as well as federal survey data in order to compile policy relevant, but difficult to access, information about the Medicaid and CHIP programs into one comprehensive tool.
The Medicaid and CHIP Payment and Access Commission (MACPAC) recently released the 2018 version of its Medicaid and CHIP Data Book. This data book is a collection of federal and state statistics regarding the Medicaid and CHIP programs that are compiled by MACPAC from multiple data sources on key topic areas including Medicaid and CHIP eligibility, enrollment, and expenditures, as well as beneficiary health, service use, and access to care. An excellent resource, the data book draws on a wide variety of data sources including Medicaid administrative data (e.g., CMS-64 data, MSIS data, Medicaid Managed Care enrollment reports, etc.) as well as federal survey data in order to compile policy relevant, but difficult to access, information about the Medicaid and CHIP programs into one comprehensive tool.
SHADAC is excited to be among the contractors that contributed to this product, providing MACPAC with estimates from the National Health Insurance Survey (NHIS) and the Medical Expenditure Panel Survey (MEPS) that highlight individual enrollment, primary source of insurance coverage, and service use and access to care with breakdowns available by age, demographics, and health characteristics. SHADAC produced these estimates using data for years 2016 and 2017, which are the latest available respectively for each survey.
For additional information on data methods and sources used in the data book, see MACPAC’s Technical Guide to MACStats, which provides supplementary information to help readers interpret the exhibits in the MACStats tables and figures as well as to understand the data sources and methods used.
Publication
Housing Affordability Matters: Measuring and Addressing the Burden of Unaffordable Rents (Infographics)
An analysis by SHADAC examines housing affordability, looking specifically at the percent of rental households that spend more than 30% of their monthly income on rent. This measure is now available on SHADAC’s State Health Compare for all states from 2012 through 2017, and can be broken down by household income, Medicaid enrollment, race/ethnicity, and disability status.[1]
Background
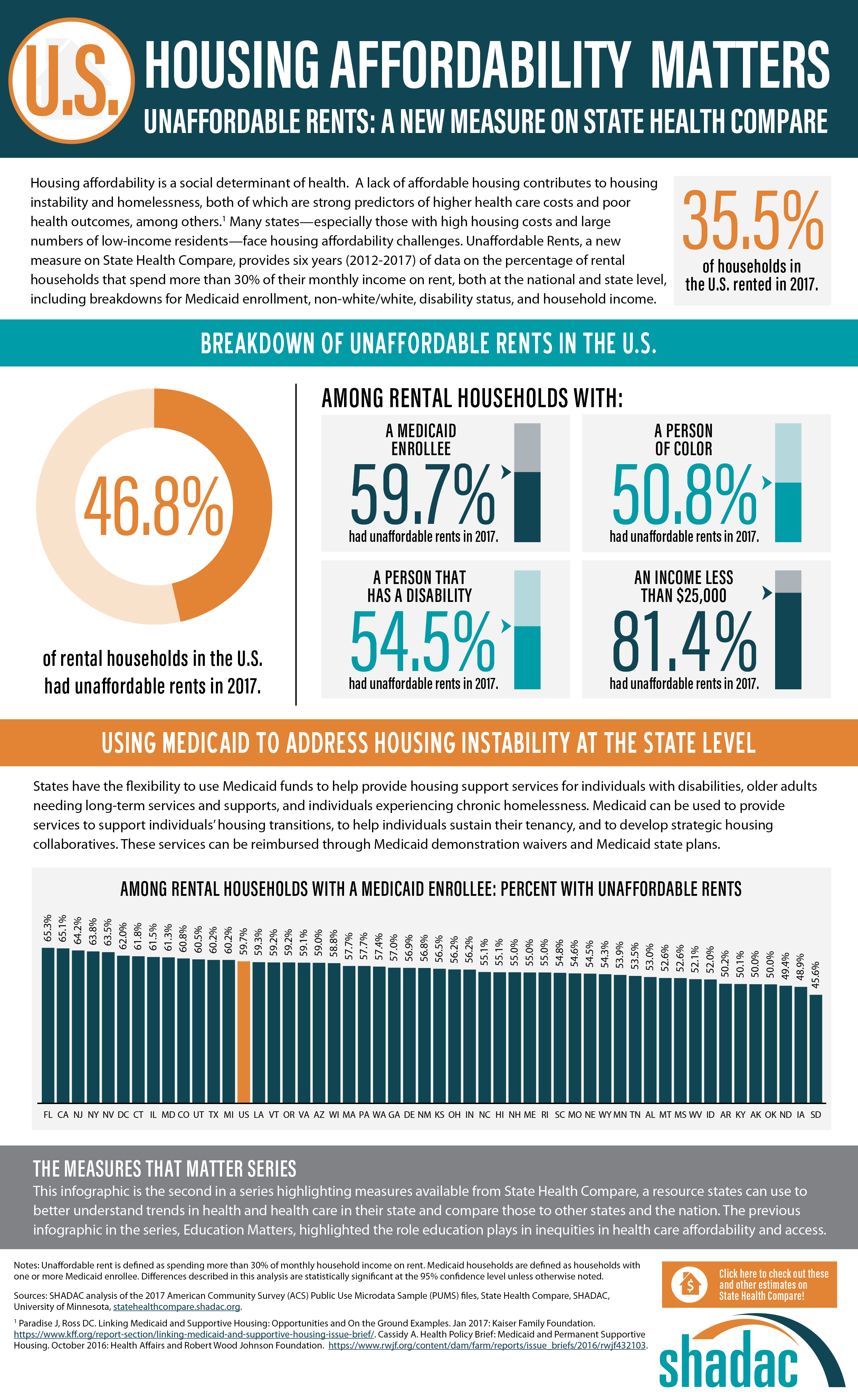
SHADAC analyzed a key social determinant of health factor—housing affordability. A lack of affordable housing contributes to housing instability and homelessness, both of which are strong predictors of higher health care costs and poor health outcomes, among others.[2] Many states—especially those with high housing costs and large numbers of low-income residents—face housing affordability challenges.
Breaking Down the Issue of Unaffordable Rents
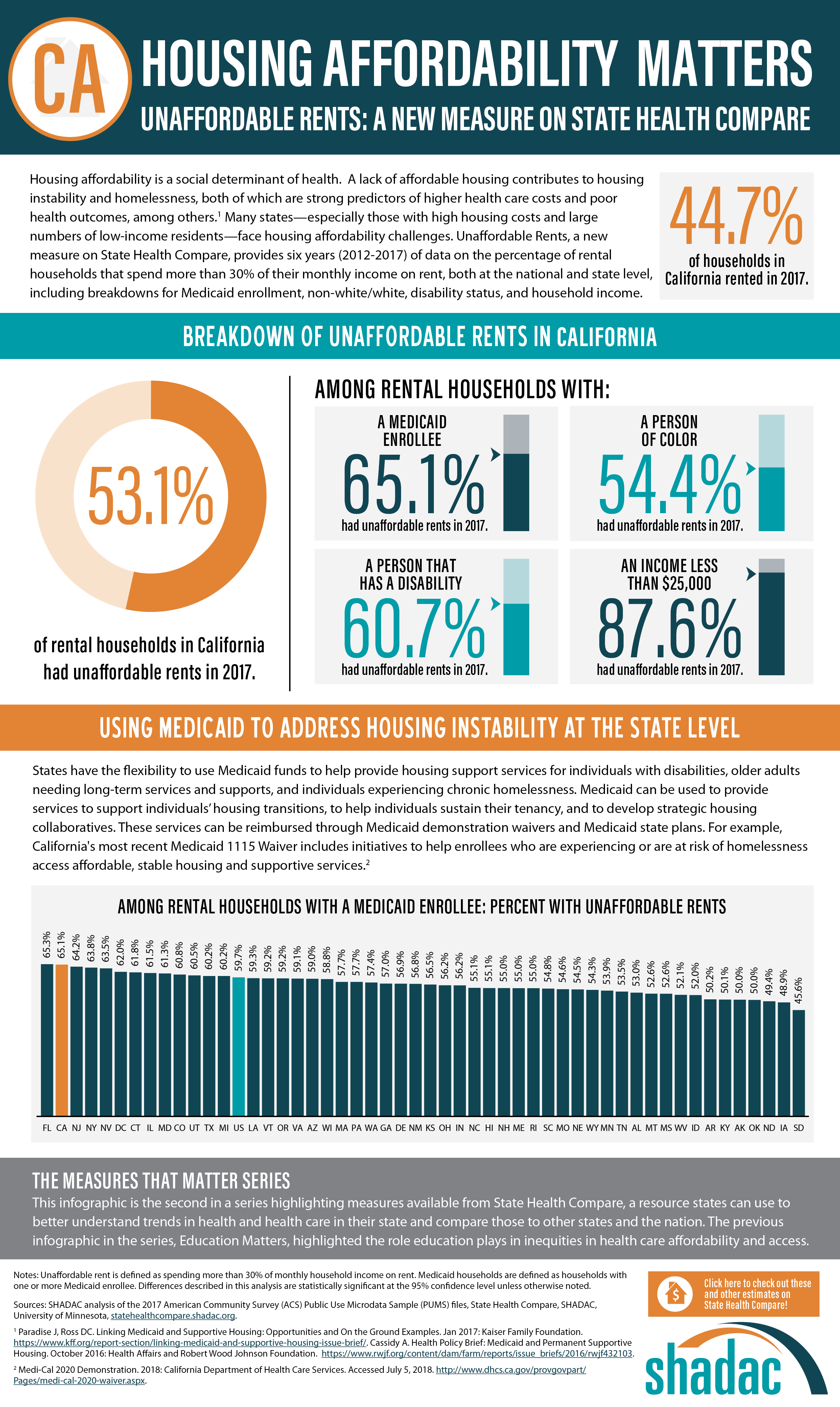
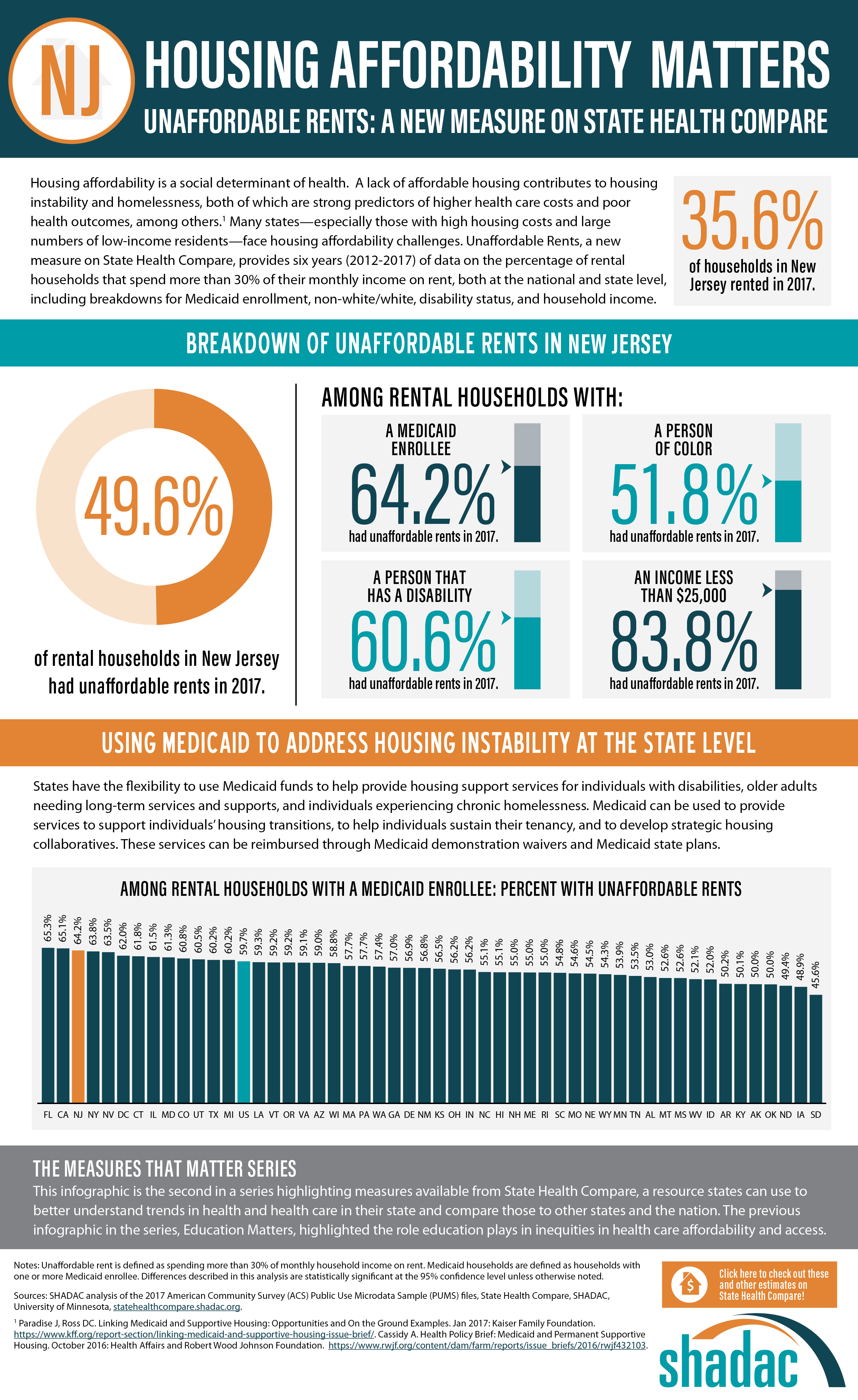
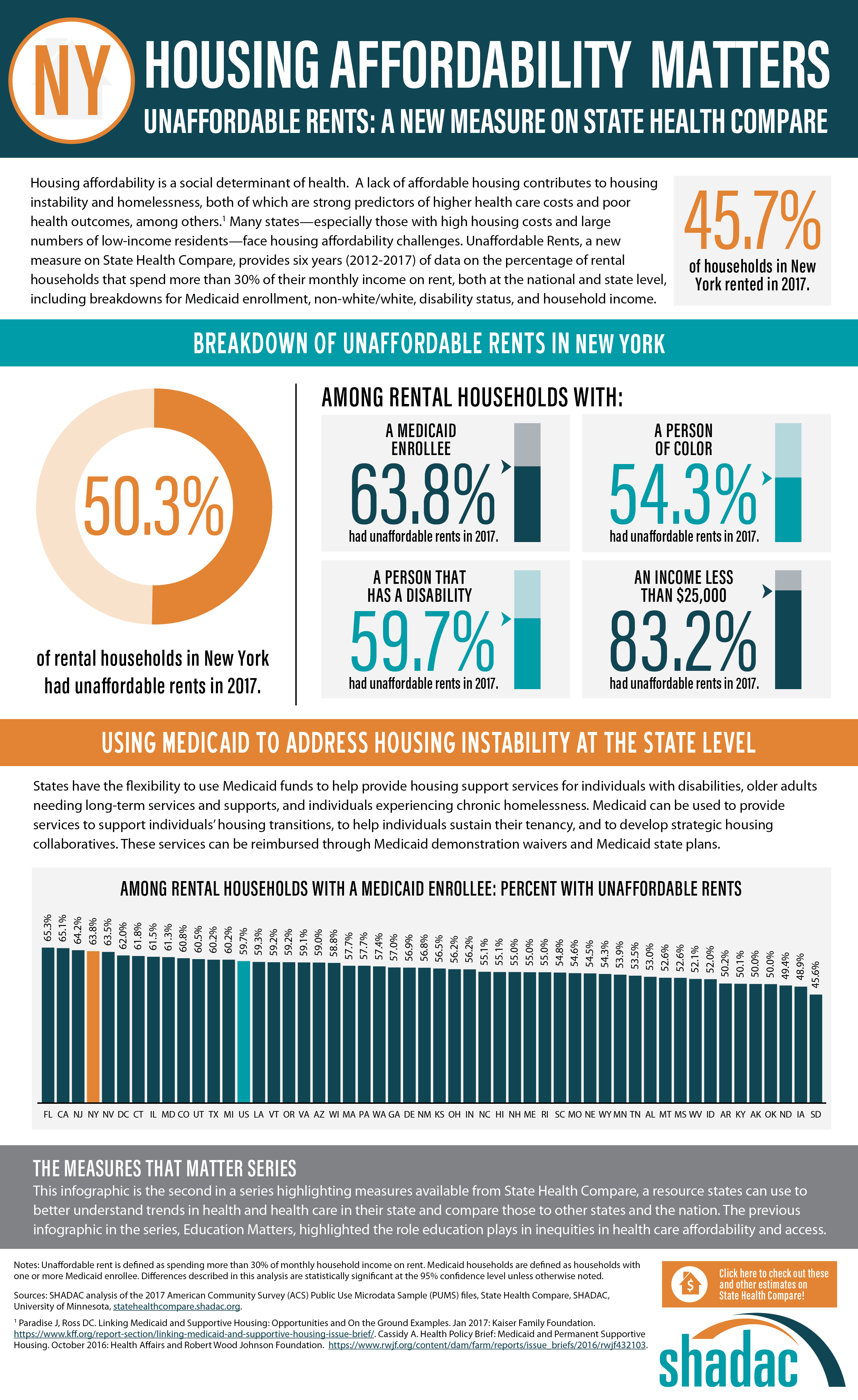
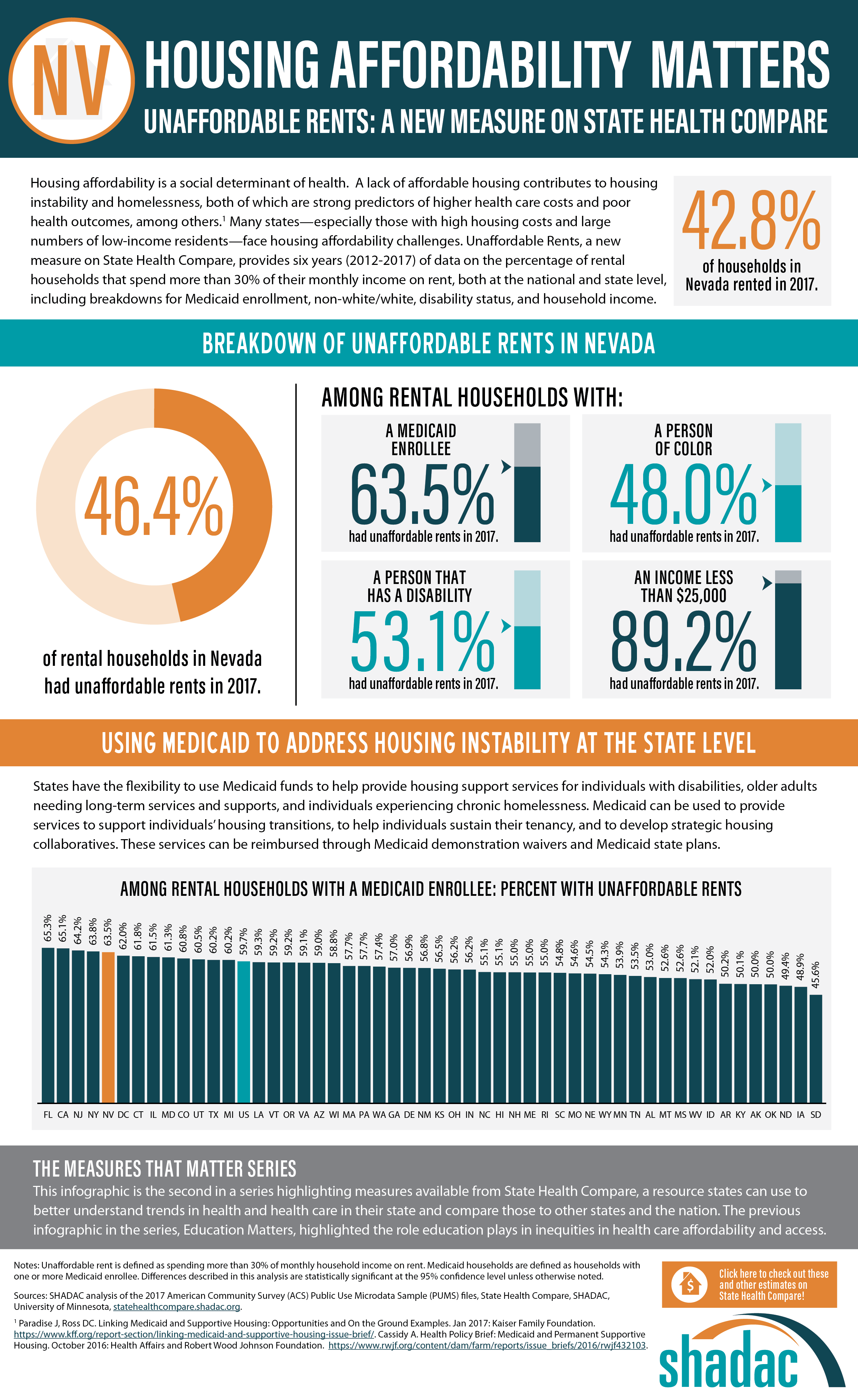
SHADAC looked at the percent of cost-burdened rental households in each state in 2017, examining unaffordable rents overall while also analyzing unaffordable rents among rental households with: a Medicaid enrollee, a person of color, a person that has a disability, and an income of less than $25,000. The infographic presented here shows these estimates for the U.S. SHADAC researchers have also created state infographics for the five states with the highest percentages of unaffordable rents among rental households that had a Medicaid enrollee—Florida (65.3%), California (65.1%), New Jersey (64.2%), New York (63.8%), and Nevada (63.5%).

Discussion: How State Medicaid Policy Can Alleviate the Burden of Unaffordable Rents
Since recent attention has been given to the idea of using Medicaid to address housing instability at the state level, the rate of unaffordable rents among rental households with Medicaid enrollees (59.7% nationally) is a particularly salient estimate, indicating that a substantial portion of this population could benefit from such efforts.
Though federal law directly prohibits federal-level matching of state Medicaid spending on housing (excepting nursing home facilities, which are already specified as a Medicaid coverage benefit), states can use Medicaid demonstration waivers and State Plan Amendments to leverage federal dollars for a wide range of housing-related services and activities, including support services for individuals with disabilities, older adults needing long-term services and supports, and individuals experiencing chronic homelessness. Medicaid can also be used to provide services to support individuals’ housing transitions, to help individuals sustain their tenancy, and to develop strategic housing collaboratives. In addition, several states, in an effort to integrate their separate yet related Medicaid and housing programs, have begun to reorganize part or all of their Medicaid delivery systems into accountable care organizations (ACOS) for more ease in using Medicaid dollars for non-medical “flexible services,” which include housing supports.[3]
Visit SHADAC and State Health Compare for More
The infographics presented here are part of SHADAC’s “Measures That Matter” product series. This series highlights measures available from State Health Compare, a web tool that states can use to explore measures related to health and health care within and across states and the nation.
The previous infographics in the series, “Education Matters,” highlighted the role education plays in inequities in health care affordability and access. Learn more about this analysis here.
Learn more about the estimates used in this analysis, as well as other measures related to social determinants of health, at State Health Compare.
[1] SHADAC. Analysis of the 2017 American Community Survey (ACS) Public Use Microdata Sample (PUMS) files. State Health Compare. statehealthcompare.shadac.org.
[2] Cassidy A. (2016). Health Policy Brief: Medicaid and Permanent Supportive Housing. Health Affairs and Robert Wood Johnson Foundation. https://www.rwjf.org/content/dam/farm/reports/issue_briefs/2016/rwjf432103.
[3] Paradise J, Ross DC. (2017). Linking Medicaid and Supportive Housing: Opportunities and On the Ground Examples. Kaiser Family Foundation. http://files.kff.org/attachment/Issue-Brief-Linking-Medicaid-and-Supportive-Housing-Opportunities-and-On-the-Ground-Examples.
Blog & News
SHADAC Examines Medicaid Eligibility, Enrollment, and Renewal in Six States – MACPAC Contractor Report
December 5, 2018: SHADAC recently conducted an assessment for the Medicaid and CHIP Payment and Access Commission (MACPAC) regarding Medicaid eligibility, enrollment, and renewal processes and systems in six study states—Arizona, Colorado, Florida, Idaho, New York, and North Carolina.
SHADAC recently conducted an assessment for the Medicaid and CHIP Payment and Access Commission (MACPAC) regarding Medicaid eligibility, enrollment, and renewal processes and systems in six study states—Arizona, Colorado, Florida, Idaho, New York, and North Carolina.
This assessment sheds light on the different choices each of the study states has made regarding structuring their Medicaid programs and the continued implementation of the Patient Protection and Affordable Care Act’s (ACA) requirement of Medicaid eligibility simplification, along with state priorities.
About the Study
SHADAC’s study sought to both understand how the selected states—with varied Medicaid policy, program priorities, and ages and capabilities of their eligibility systems—enacted different approaches to streamlining their Medicaid enrollment and renewal processes for individuals whose income eligibility is based on Modified Adjusted Gross Income (MAGI), and to assess the extent to which states were achieving desired goals such as program efficiency and a simplified beneficiary experience.
SHADAC used a multi-case study methodology and key informant interviews with 48 individuals representing state and local agencies and advocacy organizations to collect data on eligibility, enrollment, and renewal processes and systems for MAGI Medicaid populations. MACPAC was specifically interested in auto-enrollment and auto-renewal practices for MAGI Medicaid, the use of electronic data sources to verify beneficiary information, and the degree to which MAGI Medicaid enrollment and renewal is integrated with enrollment and renewal for non-MAGI Medicaid and other public benefit programs. SHADAC found that some states prioritized real-time, no-touch enrollment and renewal, while others prioritized eligibility worker involvement. All study states, however, focused on the transition to MAGI-based eligibility determinations and the use of electronic data sources to verify beneficiary information called for under the ACA.

Key Themes
Interview responses across the six states revealed several key themes related to Medicaid program and beneficiary experiences:
- Multi-benefit online applications enhanced beneficiary access to programs and reduced burden, but back-end eligibility systems are complicated to maintain.
- Electronic data interfaces facilitated high rates of real-time eligibility determinations, auto-renewal, and reduced churn.
- Robust rules engines were critical to support successful streamlined eligibility determinations, but workers still need to understand policy.
- Complex and varied programs rules remained a challenge for integration of MAGI Medicaid and other programs.
- Despite streamlined application processes, demand for enrollment assistance was high.
Areas of Ongoing Activity
The work of study states to accurately and efficiently enroll and renew Medicaid eligible populations into the program is not static, but rather focused on continuous improvement over time. Areas of ongoing activity include the following:
- Monitoring of Medicaid and related policy changes continues. Respondents were closely monitoring potential Medicaid policy changes in their states, such as Medicaid expansion proposals in Idaho and proposed Medicaid work requirements in Arizona.
- Efforts to improve beneficiary and inter-agency correspondence are important and ongoing. Four of the study states (Arizona, Colorado, Florida, New York) reported beneficiary confusion arising from correspondence about eligibility determination and renewal, and three of these states (Colorado, Florida, New York) reported plans to improve this correspondence. Half the study states also reported ongoing efforts to improve inter-agency correspondence as well.
- States continue to invest staff resources and funding to improve application and eligibility system infrastructure. All six states are currently working to increase the usability of their application platforms and enhance their eligibility systems—shifting away from legacy mainframe systems toward rules-based systems and modular, cloud-based platforms.
Related Content: MACPAC Summary Issue Brief
Publication
Assessment and Synthesis of Selected Medicaid Eligibility, Enrollment, and Renewal Processes and Systems in Six States
 This SHADAC contractor report was produced for the Medicaid and CHIP Payment and Access Commission (MACPAC). The purpose of the analysis was to examine Medicaid eligibility, enrollment, and renewal practices in six states in light of the Affordable Care Act goals of making the Medicaid program more efficient; reducing complexity and effort for enrollees and program administrators; and integrating Medicaid with the health insurance exchanges. The report summarizes how MAGI Medicaid populations apply to and are determined eligible for the Medicaid program in the study states, and it describes the study states’ approaches to streamlining enrollment and renewal for these populations, common themes among the states, and the states’ future plans to further streamline enrollment and renewal.
This SHADAC contractor report was produced for the Medicaid and CHIP Payment and Access Commission (MACPAC). The purpose of the analysis was to examine Medicaid eligibility, enrollment, and renewal practices in six states in light of the Affordable Care Act goals of making the Medicaid program more efficient; reducing complexity and effort for enrollees and program administrators; and integrating Medicaid with the health insurance exchanges. The report summarizes how MAGI Medicaid populations apply to and are determined eligible for the Medicaid program in the study states, and it describes the study states’ approaches to streamlining enrollment and renewal for these populations, common themes among the states, and the states’ future plans to further streamline enrollment and renewal.
Individual Case Study Reports
- Eligibility, Enrollment, and Renewal: Arizona Case Study Findings
- Eligibility, Enrollment, and Renewal: Colorado Case Study Findings
- Eligibility, Enrollment, and Renewal: Florida Case Study Findings
- Eligibility, Enrollment, and Renewal: Idaho Case Study Findings
- Eligibility, Enrollment, and Renewal: New York Case Study Findings
- Eligibility, Enrollment, and Renewal: North Carolina Case Study Findings
About the Study
SHADAC’s study sought to both understand how the selected states—with varied Medicaid policy, program priorities, and ages and capabilities of their eligibility systems—enacted different approaches to streamlining their Medicaid enrollment and renewal processes for individuals whose income eligibility is based on Modified Adjusted Gross Income (MAGI), and to assess the extent to which states were achieving desired goals such as program efficiency and a simplified beneficiary experience.
SHADAC used a multi-case study methodology and key informant interviews with 48 individuals representing state and local agencies and advocacy organizations to collect data on eligibility, enrollment, and renewal processes and systems for MAGI Medicaid populations. MACPAC was specifically interested in auto-enrollment and auto-renewal practices for MAGI Medicaid, the use of electronic data sources to verify beneficiary information, and the degree to which MAGI Medicaid enrollment and renewal is integrated with enrollment and renewal for non-MAGI Medicaid and other public benefit programs. SHADAC found that some states prioritized real-time, no-touch enrollment and renewal, while others prioritized eligibility worker involvement. All study states, however, focused on the transition to MAGI-based eligibility determinations and the use of electronic data sources to verify beneficiary information called for under the ACA.
Key Themes
Interview responses across the six states revealed several key themes related to Medicaid program and beneficiary experiences:
- Multi-benefit online applications enhanced beneficiary access to programs and reduced burden, but back-end eligibility systems are complicated to maintain.
- Electronic data interfaces facilitated high rates of real-time eligibility determinations, auto-renewal, and reduced churn.
- Robust rules engines were critical to support successful streamlined eligibility determinations, but workers still need to understand policy.
- Complex and varied program rules remained a challenge for integration of MAGI Medicaid and other programs.
- Despite streamlined application processes, demand for enrollment assistance was high.
Areas of Ongoing Activity
The work of study states to accurately and efficiently enroll and renew Medicaid eligible populations into the program is not static, but rather focused on continuous improvement over time. Areas of ongoing activity include the following:
- Monitoring of Medicaid and related policy changes continues. Respondents were closely monitoring potential Medicaid policy changes in their states, such as Medicaid expansion proposals in Idaho and proposed Medicaid work requirements in Arizona.
- Efforts to improve beneficiary and inter-agency correspondence are important and ongoing. Four of the study states (Arizona, Colorado, Florida, New York) reported beneficiary confusion arising from correspondence about eligibility determination and renewal, and three of these states (Colorado, Florida, New York) reported plans to improve this correspondence. Half the study states also reported ongoing efforts to improve inter-agency correspondence as well.
- States continue to invest staff resources and funding to improve application and eligibility system infrastructure. All six states are currently working to increase the usability of their application platforms and enhance their eligibility systems—shifting away from legacy mainframe systems toward rules-based systems and modular, cloud-based platforms.
Related Content: MACPAC Summary Issue Brief

