The Intersection of Medicaid and Equity
The Intersection of Medicaid and Equity
Medicaid is a critical component of the American health care system, providing coverage for approximately 72 million people, of which a little more than 47% are children. Research shows that Medicaid improves access to acute and preventive care while reducing child and adult mortality rates. With the passing and implementation of the Affordable Care Act’s (ACA) Medicaid expansion, Medicaid has increased coverage rates, improved health status, and provided economic opportunity for states.
Additionally, through its policy, financial, and programmatic levers, the Medicaid program is uniquely situated to address the inequities experienced by the program’s diverse population of enrollees. Key to these efforts to advance equity is the availability of comparable programmatic and performance data to identify and track progression in closing the gaps in health outcomes for populations across multiple states.
This page highlights some of SHADAC’s important work that examines the intersectional crossroads between equity, health-related data, and state Medicaid programs. Read on to learn more and access important reports, documents, and resources from our recent projects.
The Medicaid Equity Monitoring Tool Project (2021-2025)
With support from the Robert Wood Johnson Foundation (RWJF), researchers at the State Health Access Data Assistance Center (SHADAC) led a project designed to assess whether a comparative data tool would be useful to state Medicaid programs, policymakers, advocates, and others by providing information and opportunities for structural change to improve health equity for people enrolled in Medicaid.
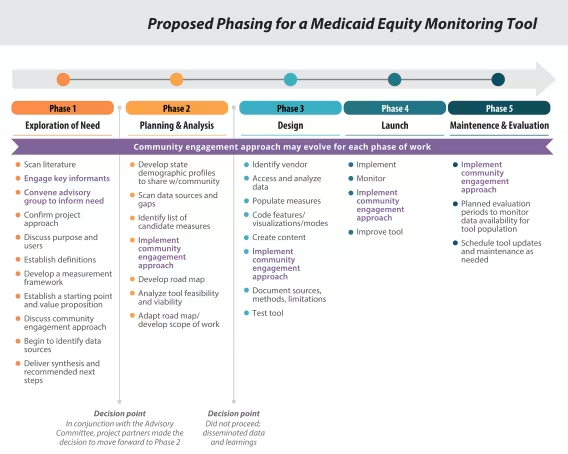
Called the “Medicaid Equity Monitoring Tool Project,” the following paragraphs provide an overview of the project’s multiple phases, including our work with partner organizations.
Our goal was to identify a set of key equity-related indicators and understand whether populating them into a centralized “Medicaid Equity Monitoring Tool” could be a helpful, feasible, and reliable way of tracking and advancing health equity in Medicaid. We did not seek to replicate other state-level data dashboards or repositories, but rather to create a tool that would serve as an easily digestible and equity-focused comparative data resource that could be used in a variety of ways, including as:
- A monitoring tool for individual states to set goals and assess progress toward achieving health equity goals in Medicaid;
- A catalyst for state-led health equity initiatives and policies;
- A discovery tool to help states learn about program actions in other states that would help advance health equity;
- A facilitation tool that would spur conversations in communities about what’s working and what’s not, or where new data are needed.
Project Timeline and Learnings
A large part of the initial work plan included concerted efforts to account for the purposeful invitation and involvement of a diversity of voices, including community members, health equity experts and scholars, data specialists, and other stakeholders. As such, we recruited and convened an Advisory Committee to guide the project throughout our first phase and advise us about whether and how a Medicaid Equity Monitoring Tool could be most useful and for whom.
Our main task of building an accessible, flexible, Medicaid member-centered tool that would allow users to monitor health equity related activities while also holding state Medicaid programs accountable for actionable solutions to equitable improve health and well-being in communities across all 50 states was ambitious in both scope and scale. As such, this project was planned to span multiple years and multiple phases of work.
Even so, one of the first lessons that SHADAC and project partner RACE for Equity learned is that the pace of project work needed to vastly slow down. Resultantly, the SHADAC team began to adapt project schedules and pivot course in order to better respond to Advisory Committee feedback and act on their requests in near-real-time. A more organic and collaborative work process began to develop at this stage; the SHADAC team and the Advisory Committee worked in consensus to identify eight key areas that we felt were foundational to build a Medicaid Equity Monitoring Tool. These became our guiding “project principles.”
Project Principles

Accountability: There is a need for a member-centered data resource for the purpose of monitoring health equity activities and outcomes.
Intersectionality: Data and perspectives from multiple communities should be considered in assessing Medicaid’s ability to advance equity.
Root Causes: The tool must highlight the root causes of inequities in the health care system and how they are connected to the Medicaid system.
Community Engagement: Centering member voices should be a primary focus in tool planning, development, and sustainability.
Member Experience: The tool should amplify self-reported data to showcase members’ experiences with Medicaid.
Visibility: The tool should identify where inequities exist, how they evolve over time, what actionable measures states are taking to address them, and areas in which more could be done.
Foundational Data: The collection of demographic data for traditionally marginalized populations—including race, ethnicity, sexual orientation, gender identity, disability, and primary language—should be improved and standardized, and current data gaps must be addressed.
Use for Good: Data collected from this tool should be used for good, avoiding the potential to support a harmful narrative around Medicaid.
Working through the complexities of our early attempts to define a measurement framework for a Medicaid Equity Monitoring Tool and scan for health equity activities by state taught project members the need to give fuller consideration to the upstream and root causes of inequities and how those would be layered into tool population and build processes.
Project Phase 1
In the first of five originally planned project phases, SHADAC researchers worked concurrently to: conduct environmental scans; engage stakeholders; develop a measurement framework for advancing health equity in the Medicaid program; and define parameters for Medicaid health equity measurement concepts. We also made sure to conduct each of these activities in regular consultation with key informants regarding our progress.
At various stages over the year-long course of the project’s first phase, SHADAC hosted three virtual convenings of the Advisory Committee. We also held invited and ad hoc conversations with several key partners and informants to discuss a number of aspects, including the measurement framework, priority measurement concepts and populations of interest, and value proposition for a potential first-iteration tool.
At the conclusion of Phase 1, SHADAC synthesized the learnings from our data scans along with feedback and proposals on tool development from the Advisory Committee and designed a prospective wireframe. This wireframe was a two-dimensional layout of a product designed to garner response on content and usability, and served as an example of what content and features a potential tool could include.
You can see that wireframe along with other resources created during this phase below.
Phase 1 Product Highlights
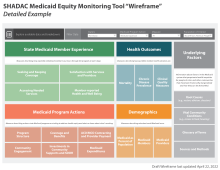
Member-Centered Framework Health Equity Activities State Scan Wireframe: Detailed Example
Project Phase 2
In the second phase, SHADAC conducted several planning activities to inform discussions of tool viability and decision making regarding next steps in tool development. In addition to SHADAC’s continued involvement of and communication with former Advisory Committee members and other subject matter experts and potential end users in project progress, SHADAC focused on two distinct yet equally important components of our work scope. Each is described in greater detail in the following paragraphs.
1) Identified and collaborated with a community partner to engage directly with Medicaid member communities
Based on our discussions with the Phase 1 Advisory Committee and in accordance with their recommendations, SHADAC recommended to our project partner RWJF that another organization be selected to serve in the crucial role of leading community member engagement..
After a lengthy search process, Health Leads, an organization that focuses on partnering with communities and health systems to discover and address societal and systemic causes of inequity that impact health and disease, was selected by RWJF as our project partner for the second phase. The team felt that Health Leads would bring a wealth of concrete knowledge and experience in the field of authentic community engagement, as well as offer a national perspective.
Beginning in June 2024, Health Leads, in conjunction with SHADAC, embarked on a process to recruit, engage, and directly listen to the lived experiences of Medicaid members and their families regarding their perspective on the inequities they experience in the program. Wanting to hear from a diverse representation of voices, Health Leads created a system whereby individuals from three states with very different Medicaid programs (California, New York, and Texas), many with vastly different demographic makeup (e.g., age, sex, income levels, race and ethnicity, and others), were selected to be part of these regional community groups. This work is currently ongoing, and we look forward to sharing more about the outcomes and learnings with our project partners and communities soon.
2) Performed data scans to understand what available data measures currently exist to populate a tool
SHADAC was able to conduct data scans for three of the five proposed wireframe “domains” (i.e., colored boxes from the Tool’s Wireframe created in Phase 1) in order to understand what data sources might be available to populate individual measures and identify gaps in this data. Those three domains are Medicaid Member Experience, State Program Actions, and Underlying Factors. In the paragraphs below, we offer a more in-depth picture of the studies and scans that were employed for each domain. In addition, SHADAC has mocked up state demographic profiles to demonstrate how recent federal survey data could be analyzed and displayed to describe the diverse populations served by state Medicaid programs.
SHADAC Medicaid State Demographic Tool Mockup (FL, NY, TX)
Medicaid Member Experience
The decision to begin with Medicaid Member Experience came from a variety of sources, including takeaways from meetings with our Phase 1 Advisory committee, guiding project principles regarding our continued commitment to centering the experience of Medicaid community members, and SHADAC’s own prior experience and knowledge regarding survey data and availability of potential measures.
From this work, we produced a pair of related resources: the “State Medicaid Member Experience Quantitative Data Scan” and the companion “State Medicaid Member Experience Qualitative Data Scan.” Each of these highlights key sources (survey data in the former and research studies in the latter) that held the greatest potential for measure population in this area, while also intentionally pointing to critical gaps in availability and existence of current, relevant sources and measures (including highlighting the lack of data stratification in surveys for key demographic groups and lack of longitudinal studies in qualitative research). SHADAC researchers also included several proposals for addressing quantitative gaps and absences, providing suggestions for improving current data collection efforts/programs as well as implementing new data collection methods.
Program Actions
Our Phase 1 Advisory Committee envisioned the “Program Actions” section of the tool would display measures describing the actions state Medicaid programs are taking to address health equity and what is known about what is working. With these concepts in mind, SHADAC researchers approached a scan of Program Actions-related measures using two different methods. SHADAC conducted a broad scan aimed at finding any and all available data sources that could provide related measures to populate a tool with data for all 50 states and could later be pared down to a more realistic and relevant number of measures to display within a tool. In addition, SHADAC completed a more targeted literature review of sources that provided demonstrable evidence of state Medicaid program action success in addressing barriers to health equity and reducing disparities.
From the results of these two scans, a compendium of state Medicaid program action data sources has been created by SHADAC researchers, and can be found here and is linked below.
Underlying Factors
This section in the proposed wireframe went through several conceptual iterations before we arrived at an understanding that this domain needed to be populated with information about compounding factors in the Medicaid system that perpetuate health inequities and erect barriers to health for people of color and other communities that have been historically marginalized and how they can be dismantled. As a starting point, SHADAC created an “Annotated Bibliography” of academic research and grey literature sources that explain and provide analysis for the underlying factors and root causes that may contribute to inequities in Medicaid. These topics are complex and intersectional, and our researchers scanned for recent (2018 and onward) and relevant sources that would not only help readers understand the varied and interconnecting root causes of Medicaid inequities, but would also identify and uplift potential solutions.
The Annotated Bibliography is currently structured into five separate but related sections: Systemic Racism; Systemic/Structural Ableism; Sexual Orientation, Gender Identity, and Gender Affirming Care Discrimination; Reproductive Oppression in Health Care; and Impact on Vital Community Conditions.
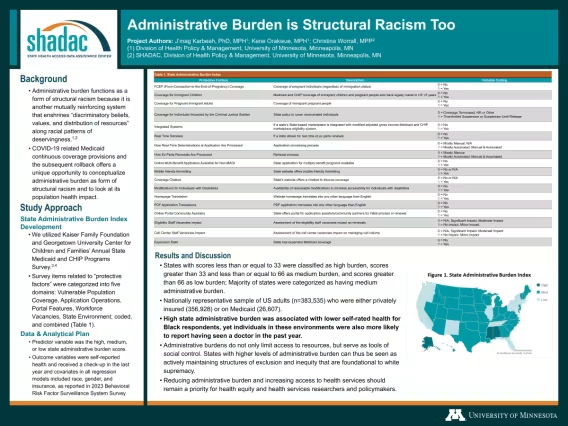
In related work, we consulted with a professor in the University of Minnesota School of Public Health regarding contextual factors in understanding inequity in Medicaid, and from our discussions work has progressed on an assessment of the relationship between administrative burden in Medicaid and select health outcomes. Both a presentation at Academy Health's Annual Research Meeting in June 2025 and a forthcoming journal article are currently in production.
Phase 2 Product Highlights




Annotated Bibliography Conversations with Experts Member Experience Quantitative & Qualitative Scans Program Actions Scan
In related work, we consulted with a professor and doctoral student in the University of Minnesota School of Public Health regarding contextual factors in understanding inequity in Medicaid, and from our discussions work has progressed on an assessment of the relationship between administrative burden in Medicaid and select health outcomes. Find a version of their June 2025 Academy Health Annual Research Meeting presentation on this work here, also posted below. A forthcoming journal article is currently in production.
Project Partners
Robert Wood Johnson Foundation
The Robert Wood Johnson Foundation (RWJF) is a leading national philanthropy dedicated to taking bold leaps to transform health in our lifetime. Through funding, convening, advocacy, and evidence-building, RWJF works side-by-side with communities, practitioners, and institutions to achieve health equity faster and pave the way, together, to a future where health is no longer a privilege, but a right.
RWJF was the main funding source for this project, and program officers from RWJF worked with the SHADAC and Health Leads teams to facilitate project timelines, partner organization review and selection, Advisory Committee meetings, and data gathering and member engagement processes.
RACE for Equity
R.A.C.E. for Equity was launched in 2018 with the goal to support leaders to achieve and scale measurable results through authentic and sustained community engagement. Their services include training, technical assistance and direct coaching as organizations design services, programs, policies, and/or strategic action plans.
R.A.C.E. for Equity has been a valued partner throughout this project, providing technical assistance, collaborating with SHADAC team members to develop the research principles that underpinned much of the project work, and facilitating meetings and discussions with experts throughout all phases of this work.
Health Leads
Health Leads is an organization with national reach that focuses on partnering with communities and health systems to discover and address societal and systemic causes of inequity that impact health and disease. Health Leads was brought on board during the second phase of the project to lead the work to facilitate Medicaid member and community discussions around potential data measures that would be meaningful for inclusion within a potential tool and ensure that these voices remain centered throughout all project work and processes.
Cross-Cutting Work and Future Considerations
This work builds on a body of research funded by RWJF on the important role Medicaid plays in building a “culture of health.” It also aligns with other RWJF efforts related to promoting health equity and community partnership in public health system change. Studies have shown that structural changes which remove barriers for individuals who are most impacted by them also result in removing these barriers for others. Equity benefits all of society.
While the project was originally planned to span five phases of work, recent events have precipitated a shift in focus -- away from a state-level data tool and toward protecting state Medicaid programs. So while the initial phases of this work yielded rich insights into the potential utility and considerations around a Medicaid Equity Monitoring Tool, we will not be moving forward with the development of an actual tool at this time. In addition, we have learned through our many data scans and conversations with stakeholders and potential users that such a tool as we had originally envisioned would not be feasible to build due in part to gaps in available and actionable data.
We want to underscore that the completed phases of this project have provided key insights and multiple resources on understanding the current landscape of health equity in Medicaid, and we remain committed to continue working with trusted partners in the communities Medicaid serves to find new ways of reducing barriers to equitable health outcomes.
You can always access the resources and documents on this project page. If you have any questions about this project or any of the products created as a part of it, don't hesitate to reach out to SHADAC - we would be excited to discuss the work and see how we can work together to improve Medicaid and reduce disparities.
To stay up to date on our latest projects and resources, sign up for our mailing list.