
Blog & News





Revised Childhood Vaccinations Measure on State Health Compare Shows Vaccination Rates Vary by State, Race/Ethnicity, and Insurance Coverage
January 30, 2024:Introduction
Childhood Vaccinations are an effective way to protect infants and young children from harmful diseases that can cause serious illness or death. Children are commonly vaccinated against a number of diseases, including chickenpox (Varicella), polio, hepatitis A and B, and measles, mumps, and rubella (MMR).
Despite the well-documented safety and efficacy of the vaccines, along with the endorsement of child vaccinations by the Centers for Disease Control and Prevention (CDC) and other public health authorities, rates of child vaccination lag in some portions of the United States. Monitoring trends in child vaccination rates can help explain why such gaps exist and inform efforts to improve child vaccination rates in the U.S.
A revised child vaccination measure on SHADAC’s State Health Compare (SHC) now presents annual, state-level vaccination rates for children aged 35 months, specifically the percent of those children who received the full series of recommended vaccines using data from the National Immunization Survey (NIS-Child) by survey year. This measure also presents these state-level rates by race and ethnicity, health insurance coverage type, and poverty level. In this blog post, SHADAC researchers highlight key findings from this new child vaccinations measure by race and ethnicity and type of health insurance coverage.
The Share of Children Receiving Recommended Vaccinations Has Been Relatively Stable, Though Large Variation Exists Across States
Nationally between 2017 and 2021, the share of children aged 35 months who had received the full schedule of recommended vaccinations remained relatively stable, remaining between 70% and 73% nationwide.
National Child Vaccination Rates, 2017–2021
However, while stable nationally, there was substantial state variation in the share of children who had received recommended vaccinations. For example, in 2021, the national child vaccination rate sat at 72.1%, but state-level rates ranged from as low as 56.6% in West Virginia to as high as 87.9% in Iowa. Also in 2021, six states (CT, IA, MD, MA, ND, and VT) had child vaccination rates of 80% or greater while West Virginia was the only state with a vaccination rate below 60%.
Top Five and Bottom Five State Child Vaccination Rates, 2021
| Top Five States | Iowa | 87.9% |
|---|---|---|
| Massachusetts | 85.4% | |
| Connecticut | 84.0% | |
| Vermont | 82.1% | |
| North Dakota | 81.3% | |
| United States | 72.1% | |
| Bottom Five States | West Virginia | 56.6% |
| Alaska | 61.3% | |
| Louisiana | 62.0% | |
| Arizona | 62.2% | |
| Georgia | 63.3% | |
Black Children, Hispanic/Latino Children, and Children of Other or Multiple Races Were Less Likely to Have Received Recommended Vaccinations Compared to White Children
Nationally, there were significant gaps in the share of children who had received the recommended vaccines by age 35 months by race and ethnicity.1
Non-Hispanic White children had the highest rate of vaccination at 75.5%, followed by children of multiple races or some other race (non-Hispanic) at 72.8%, Hispanic/Latino children (any race) at 69.9%, and, finally, African-American/Black children at 66.5%.
National Child Vaccination Rates by Race and Ethnicity, 2019–2021
There were also large gaps in rates of child vaccinations by race and ethnicity at the state level in 2019–2021, as shown in the table below. For example, in Michigan, African-American/Black children were nearly 30 percentage points less likely to have received the full schedule of recommended vaccinations compared to White children (49.8% vs. 79.3%). In the District of Columbia, Hispanic/Latino children were more than 20 percentage points less likely to have received the recommended vaccinations compared to White children (62.1% vs. 82.5%). And in North Dakota, children of some other race or multiple races were 20 percentage points less likely to have received the recommended vaccinations compared to White children (60.1% vs. 80.1%).
States with statistically significant gaps in child vaccination rates by race and ethnicity, 2019–2021
| State | White | African-American / Black | Hispanic / Latino | Other / Multiple Races |
|---|---|---|---|---|
| United States | 75.5% | 66.5%* | 69.9%* | 72.8%* |
| Dist. of Columbia | 82.5% | 68.1%* | 62.1%* | 70.8% |
| Georgia | 75.2% | 57.8%* | 69.8% | 70.8% |
| Illinois | 79.3% | 61.3%* | 66.9%* | 75.9% |
| Indiana | 73.1% | 66.0% | 59.1%* | 70.4% |
| Louisiana | 70.1% | 58.5%* | 69.3% | 71.9% |
| Maryland | 84.5% | 75.7%* | 71.4%* | 77.7% |
| Michigan | 79.3% | 49.8%* | 76.7% | 72.8% |
| Nevada | 76.4% | 55.8%* | 73.2% | 72.7% |
| New Jersey | 76.1% | N/A | 59.6%* | 72.2% |
| New Mexico | 76.6% | N/A | 67.7%* | 72.6% |
| New York | 69.8% | 69.0% | 67.0% | 79.5%* |
| North Dakota | 80.1% | N/A | N/A | 60.1%* |
| Oklahoma | 75.2% | N/A | 71.1% | 59.5%* |
| Rhode Island | 81.7% | N/A | 70.6%* | 83.1% |
| Tennessee | 75.9% | 49.4%* | 59.9%* | 76.6% |
| Texas | 71.0% | 61.7%* | 72.2% | 70.1% |
|
* Statistically significant difference (95% confidence level) in state estimate compared to Whites Source: SHADAC analysis of 2019–2021 NIS-Child microdata N/A indicates that data were not available or were suppressed due to statistical unreliability or small sample size |
||||
Health Insurance Coverage Matters for Rates of Child Vaccinations
Nationally, during the years 2020 through 2021, there were substantial gaps in the share of children who had received the recommended vaccinations by source of health insurance coverage. Children with private coverage alone (e.g., employer-sponsored or direct-purchase coverage) had the highest rate of vaccination coverage at 80.3%. Children with some other insurance (Children's Health Insurance Plan [CHIP] coverage, Indian Health Service [IHS] coverage, military, or some other form of insurance alone or in combination with private insurance) had a vaccination rate of 70.7%. Children with any Medicaid coverage (alone or in combination with other coverage) had a vaccination rate of 66.2%, 14 percentage points lower than private coverage. Children with no health insurance coverage (i.e., uninsured) had by far the lowest vaccination rate at 50.0%, which is more than 30 percentage points lower than children with private coverage alone.
National Child Vaccination Rates by Coverage Type, 2020–2021
That national pattern holds across the states, though due to small sample sizes, there are few available state-level estimates for children with other insurance and uninsured children. The chart below compares rates of vaccinations for children with private coverage alone and children with any Medicaid coverage. Rates of vaccinations among children with Medicaid were lowest in Alaska at 53.1% and highest in Connecticut at 81.1%. Child vaccination rates among children with Medicaid were at or below 60%in five states—AK, CO, KS, LA, and NJ—and were at or above 80% in just two states—Connecticut and Iowa. Rates of vaccinations among children with private coverage alone ranged from the lowest at 74.2% in Minnesota to the highest at 90.3% in Iowa.
In 35 states, children with any Medicaid coverage were less likely to have received recommended vaccinations compared to children with private coverage alone. Colorado had the largest percentage point gap between children with private coverage alone and any Medicaid coverage at 23.4 (82.4% vs. 59.0%), while Nebraska had the smallest gap at 1.5 percentage points (not statistically significant, 79.8% vs. 78.3%).
Data and Methods
Estimates of child vaccination rates represent the share of children aged 35 months who have received all recommended vaccinations, including the full series of DtaP, poliovirus, measles-containing, Hib, HepB, varicella, and PCV vaccines, which together provide protection against diphtheria, pertussis, tetanus, poliovirus, measles, mumps, rubella, hepatitis b, haemophilus influenza b, chicken pox, and pneumococcal infections.
Data in this post come from SHADAC’s revised Child Vaccinations measure on State Health Compare, which are based on our analysis of National Immunization Survey-Child (NIS-Child) microdata produced by the Centers for Disease Control and Prevention.
Three years of data were pooled to produce estimates by race and ethnicity; two years of data were pooled to produce estimates by coverage type. In both cases, this was done to increase sample sizes at the state level for smaller populations and to increase the number of statistically reliable state estimates. Estimates represent an average for these periods.
Note that the data source used in this analysis (NIS-Child) does not make data by more detailed race and ethnicity categories available. It is likely that these available categories conceal important differences within the aggregate groups, particularly the “some other race / multiple races” category. This group is likely to be primarily composed of children of different racial and ethnic groups in different states. Further, estimates were not available for all states for all racial and ethnic groups due to small sample sizes, even when pooling multiple data years.
Unless otherwise specified, all differences described in this analysis are statistically significant at the 95% level of significance.
1 Race lacks a genetic basis—it is socially constructed based on skin color and “apparent” physical differences. While race is socially created, it does have real social meaning and implications for health and well-being, including access to important health care services, such as vaccinations.
Blog & News

New State Health Compare estimates on Adverse Childhood Experiences aim to improve understanding of health inequities
August 28, 2023:SHADAC has posted updated estimates of the prevalence of adverse childhood experiences (ACEs) to State Health Compare. These new estimates combine six years of data from the National Survey of Children’s Health (NSCH) to enable more precise and granular estimates for smaller racial and ethnic subpopulation groups that often are under-researched due to data limitations. For instance, the new ACEs estimates include both U.S.- and state-level rates for American Indian/Alaska Native children, Asian children, and Native Hawaiian and Other Pacific Islander children, as well as Black/African American children, Hispanic/Latino children, and White children.
Earlier in 2023, SHADAC researchers Colin Planalp and Andrea Stewart published an issue brief on ACEs, explaining the relationship between potentially traumatic childhood experiences and long-term health impacts. Over the past quarter-century, an established and growing body of research has linked exposure to ACEs with a litany of health conditions that can last into adulthood, including physical health impacts, such as heart disease and diabetes, mental health conditions, and substance use disorders.
These new data build on SHADAC’s earlier work in two important ways. First, while Planalp and Stewart’s issue brief combined four years of NSCH data to allow for disaggregation of racial and ethnic groups at the U.S. and state levels, our decision to combine six years of NSCH data resulted in additional precision, which supports equity-focused analysis for demographically small populations. While that approach entails tradeoffs, such as making the data a bit less recent, we believe the advantages outweigh the disadvantages, especially for assessing the relationship between ACEs and health equity.
Second, the referenced issue brief reported estimates for one or more ACEs—a useful measure for examining the prevalence of ACEs, but this measure has limitations for understanding the implications of ACEs. Research suggests that ACEs carry a “dose effect,” meaning that exposure to one ACE carries some health risk, but exposure to multiple ACEs during childhood entails a substantially higher risk of associated health burdens. For the updated SHC estimates pooling six years of data, we were able to produce three estimates: Percent of children with zero reported ACEs, percent of children with one reported ACE, and percent of children with multiple (i.e., two or more) ACEs.
As with SHADAC’s earlier work on the topic, these new estimates of ACEs prevalence illustrate clear health disparities. For instance, American Indian/Alaska Native children had the highest reported exposure to multiple ACEs, at almost four in 10 children, while Asian children had the lowest, at less than one in 10 children (see table below).
Percent of Children Exposed to Two or More ACEs by Race/ethnicity, 2016-2021
| Race/ethnicity group | Percent |
|---|---|
| American Indian/Alaska Native | 36.5% |
| Asian | 5.9% |
| Black/African American | 27.4% |
| Hispanic/Latino | 19.0% |
| Native Hawaiian/Other Pacific Islander | 19.0% |
| White | 16.4% |
| Other/Multiple Races | 24.6% |
Sources: SHADAC analysis of 2016-2021 National Survey of Children’s Health
Together with research linking ACEs to long-term health burdens, these new estimates on SHADAC’s State Health Compare bolster our understanding of how childhood experiences influence health equity: By intervening to reduce the prevalence of ACEs and eliminate disparities in their prevalence, the U.S. might not only improve the lives of children now but improve their health well into adulthood and enhance health equity across our society.
Related Reading
Supporting Families: Associations between Neighborhood Support and Child Health Outcomes Blog
The Kids Aren't Alright: Adverse Childhood Experiences and Implications for Health Equity, Issue Brief
Neighborhood Support Matters for Child Health, Blog
Blog & News
Supporting Families: Associations between Neighborhood Support and Child Health Outcomes
August 24, 2023:Background
The circumstances of peoples’ lives have great influence over their health, often much more than genetics or access to health care—a concept known as “social determinants of health.” One such social determinant is social capital, which includes the networks of relationships that people rely on for help and to help others to exist and function in society.
We wanted to understand how one measure of social capital—living in a supportive neighborhood—may affect people’s health status and other risk factors. Our study focused on children, using data from the National Survey of Children’s Health (NSCH), which asks parents about their kids’ health, certain risk factors, and questions about their perceptions of social support in their neighborhoods.
Parents reported the extent to which they agreed—from “strongly disagree” to “strongly agree”—with three related questions about giving and receiving help in their neighborhoods. Children were defined as living in a supportive neighborhood if their parents agreed with all three questions and “strongly agree” with at least one of them:
- People in this neighborhood help each other out.
- We watch out for each other's children in this neighborhood.
- When we encounter difficulties, we know where to go for help in our community.
Study approach
The NSCH includes nationally representative data for children age 0-17 in all 50 states. This survey provides important information on child and family characteristics, as well as parental perceptions of neighborhood support. In the NSCH, children with special health care needs are identified with a five-item screener based on whether they have health needs such as prescription medication or specialized therapies for a condition expected to last longer than 12 months. We assessed which groups of children were more likely to live in supportive neighborhoods, and how this support correlated with child health and access to health care. We pooled 2020-2021 data (n=88,891) to enhance our ability examine the relationship between neighborhood support and the health status of children with greater precision and reliability.
To understand how supportive neighborhoods relate to children’s health, we focused on five child health measures including access to and use of health care, and exposure to a set of health risk factors known as adverse childhood experiences (ACEs). The measures were based on parents’ responses:
Health status
- Parent-reported child health status, measured as fair/poor vs. excellent/very good/good
- Parent-reported oral health status, measured as fair/poor vs. excellent/very good/good
Health care access and use
- Emergency room (ER) visit in the past year (one or more)
- Any past-year forgone health care in the past year (medical, dental, vision, or mental health care)
ACEs
- Exposure to two or more ACEs. This composite measure was based on parent recollection for a list of potentially traumatic experiences in the child’s household, such as difficulty affording basic necessities, divorce, death of a parent, exposure to violence in the home or neighborhood, and living with someone experiencing mental illness or substance abuse.
Findings
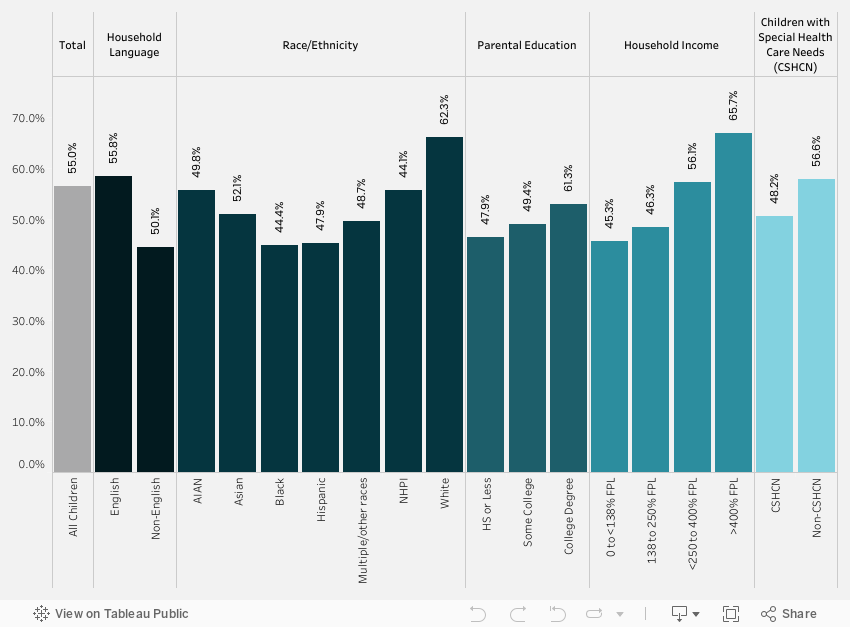
We found that slightly over half (56.4%) of all children lived in neighborhoods that their parents reported as supportive (Figure 1). The lowest rates of children living in supportive neighborhoods were reported for subgroups of children who were black (44.8%) or Hispanic (45.3%); who lived in households in which English was not the primary language (44.5%); who had family incomes below the federal poverty level (45.6%); or whose parents had an education of high school or less (46.3%). Children with special health care needs were also less likely to live in supportive neighborhoods (50.5%). The differences in children’s neighborhood support by race/ethnicity, household language, income, education, and special health care needs were significant and consistent in our tabulation of population rates and multivariate analysis.
Figure 1. Neighborhood support by child characteristics
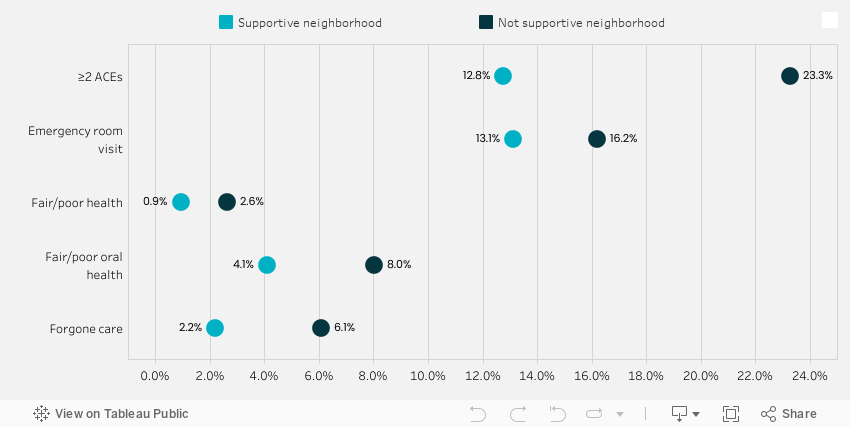
Importantly, we also found that children living in supportive neighborhoods had fewer ER visits, better access to health care (less forgone health care); better health status (less likely to have fair/poor health and oral health); and a lower prevalence of having two or more ACEs (Figure 2). Exposure to multiple ACEs is a risk factor for a number of long-term health conditions. The significant association between neighborhood support and better child outcomes shown in Figure 2 remained consistent in multivariate analysis.
Figure 2. Rates of child outcomes by neighborhood support
Conclusions
Our study highlights the importance of one measure of social capital—living in supportive neighborhoods—for a range of child outcomes including ER use, forgone care, overall and oral health status, and ACEs. This research bolsters the arguments for policies that support social networks and supports in the communities where children live, such as school and community health resources.
For children, community resources are important for their long-term outcomes. Strong neighborhoods support population health in nuanced ways that go beyond a neighborhood’s more obvious features, such as parks where people can exercise and grocery stores where people can buy healthy food. For example, previous research has shown that living in supportive neighborhoods with social networks to care for kids can mitigate the negative impact of traumatic experiences on child mental health. Our study found that neighborhood support is also associated with a reduced likelihood of ACEs and a range of beneficial child health outcomes.
This analysis was originally presented at the Academy Health Annual Research Meeting in Seattle, WA, on 6.26.2023.
Related Reading
New State Health Compare estimates on Adverse Childhood Experiences aim to improve understanding of health inequities Blog
The Kids Aren't Alright: Adverse Childhood Experiences and Implications for Health Equity, Issue Brief
Neighborhood Support Matters for Child Health, Blog
Blog & News

Interventions Likely Prevented Childhood Poverty from Rising During the Pandemic
July 20, 2023:Research has shown that since the start of the COVID-19 public health crisis, aggressive government interventions, aimed at reducing broader economic fallout as well as individual-level hardship, have been largely sucessful.1 To preempt a potential increase in poverty due to pandemic-related job loss, income loss, and health insurance coverage loss, the federal government implemented policies such as a temporary Child Tax Credit (CTC), COVID-19 rescue payments, requirements for states to maintain current Medicaid enrollment and coverage, and increased SNAP (food stamp) allotments.1,2 Evidence suggests that these targeted actions may have contributed to a small but statistically significant decrease in nationwide childhood poverty between 2019 and 2021, falling from 19.1% to 18.7%, as seen in data available on SHADAC’s State Health Compare tool.
| Childhood poverty is defined as children whose household incomes are below 100% of the Federal Poverty Guidelines, which was $30,000 in 2021, for a family of four.3 |
In this blog, SHADAC presents 2021 estimates of childhood poverty at the national and state level based on our analysis of the U.S. Census Bureau’s American Community Survey (ACS) Public Use Microdata Sample (PUMS) file and compares them to 2019 data, as 2020 childhood poverty estimates were not released due to pandemic impacts on data collection. (Please see a previous blog for more technical detail.) We also highlight notable differences in childhood poverty estimates for different racial and ethnic populations.
Highlights from 2021 Data
Compared to the pre-COVID-era figures previously reported by SHADAC, 2021 estimates for childhood poverty were significantly lower both at the overall national level and in five particular states — Arizona, Connecticut, Missouri, Tennessee, and Utah — while no states saw any significant increases in their childhood poverty rates.3 These data highlight the surprising fact that childhood poverty declined at a time when many expected it to rise for the reasons highlighted above.
Childhood poverty rates remain highest in southern states, specifically in Mississippi, followed by Louisiana, New Mexico, the District of Columbia (D.C.), and Alabama. Consistent with 2019 data, states in the Northwest, Northeast, and Midwest regions tend to have the lowest rates of childhood poverty, with New Hampshire having the lowest rate at 9.0%, followed by Utah, Vermont, Minnesota, and North Dakota.
| 5 states with the lowest rates | 5 states with the highest rates | |||
| New Hampshire | 9.0% | Mississippi | 29.4% | |
| Utah | 9.1% | Louisiana | 27.7% | |
| Vermont | 9.7% | New Mexico | 27.2% | |
| Minnesota | 10.2% | District of Columbia | 27.1% | |
| North Dakota | 10.3% | Alabama | 23.8% | |
Current survey data only allow for demographic disaggregation by race and ethnicity, specifically for African American/Black, Hispanic/Latino, non-Hispanic White, and Other/Multiple Race populations. In 2021, estimates show that one-third of children (33.9%) who identified as African American/Black were living in poverty. In addition, a quarter of children (25.7%) who identified as Hispanic/Latino were living in poverty, while 16.4% of children who identified as being of Other/Multiple races and 11.6% of those who identified as White were living in poverty, respectively.
Figure 1. Percent of children considered to be poor (<100% FPG) by state, 2021
Understanding Poverty Trends Pre- and Post-Pandemic
Despite concerns that the economic consequences of the COVID-19 pandemic would increase rates of childhood poverty, data show the opposite – a small but statistically significant decline. Combined with other research that uses measures of economic well-being, this falling poverty rate suggests that targeted pandemic-era government actions likely succeeded in their efforts to prevent further hardship during this latest public health crisis.
These positive data trends are welcome news, especially given that childhood poverty can have lasting negative effects. For example, children living in poverty are twice as likely to be exposed to adverse childhood experiences, according to a February 2023 SHADAC brief on Adverse Childhood Experiences (ACEs). Childhood poverty can also contribute to both a greater likelihood of disease onset in adulthood and limited chances for socioeconomic mobility or educational opportunity.4
Conclusions
Specific pandemic-era interventions implemented by the federal government likely contributed to a drop in childhood poverty rates between 2019 and 2021. Although programs such as the Child Tax Credit were short-lived and enacted in response to the COVID-19 public health crisis, their success in helping to reduce overall childhood poverty rates bears consideration as longer-term mechanisms to address this issue. Additionally, while overall poverty rates for children declined during this time period, evidence showing disparities in childhood poverty rates by race and ethnicity remains – likely influenced by factors such as systemic racism, social marginalization, and community-level disinvestment.4 For these reasons among others, continued research, monitoring, and advocacy efforts are vital in the ongoing fight against childhood poverty.
About the Data
The measure used for these estimates, “Percent of children considered to be poor (<100%FPG),” can be accessed through SHADAC’s online data tool, State Health Compare. These estimates were produced through SHADAC’s analysis of the American Community Survey (ACS) Public Use Microdata Sample (PUMS).
References
1. Collyer, S., Hardy, B., & Wimer, C. (2023, March 1). The antipoverty effects of the expanded Child Tax Credit across states: Where were the historic reductions felt? Brookings Institute. https://www.brookings.edu/research/the-antipoverty-effects-of-the-expanded-child-tax-credit-across-states-where-were-the-historic-reductions-felt/
2. United States Census Bureau. (2023, May 2). The Impact of the 2021 Expanded Child Tax Credit on Child Poverty. https://www.census.gov/library/working-papers/2022/demo/SEHSD-wp2022-24.htm
3. State Health Access Data Assistance Center. (2023, April 18). FPG vs. FPL: What’s the Difference? SHADAC.https://www.shadac.org/news/fpg-vs-fpl-whats-difference
4. Woolf, S. H. (2017). Progress In Achieving Health Equity Requires Attention to Root Causes. Health Affairs.https://www.healthaffairs.org/doi/10.1377/hlthaff.2017.0197
Blog & News
SHADAC at the 2023 AcademyHealth Annual Research Meeting
June 1, 2023:A number of SHADAC researchers will be presenting their work at the 2023 AcademyHealth Annual Research Meeting (ARM) taking place in Seattle, WA from Saturday, June 24 to Tuesday, June 27. For details on research topics and where you can find their posters and presentations, see below.
Association of Discrimination Based on Sexual Orientation and Gender Identity with Health Care Access and Health Outcomes

Presented in “Building the Evidence on Under-Recognized Populations” session on Monday, June 26, 2023 at 1:00 PM.
Discrimination based on sexual orientation and gender identity (SOGI) represents an important barrier to health care access. Few studies have examined SOGI-based discrimination experienced in a health care setting and its association with health care access and health outcomes, including confidence in getting care and physical and mental health. Our study fills this gap by using inclusive SOGI data and correlating direct reports of discrimination with a range of health-related outcomes. Download the presentation slides here.
Authors: Natalie Schwehr Mac Arthur (Presenter), Kathleen Panas, Kathleen T. Call
Supporting Families: Associations between Neighborhood Support and Child Health Outcomes

Presented in “Child and Family Health Poster Session” on Monday, June 26th from 2:45 PM-4:00 PM.
Living in a supportive neighborhood is one measure of social capital, which is an important social determinant of health. However, few nationally representative studies have examined the relationship between neighborhood support and the health status of children, including adverse childhood experiences (ACEs). We fill this gap using nationally representative data that includes important information on neighborhood and family characteristics.
Authors: Natalie Schwehr Mac Arthur (Presenter), Colin Planalp, Lynn A. Blewett
Factors Associated with COVID-19 Symptoms Longer Than Three Months (long COVID): Evidence from the Household Pulse Survey
Presented in “Best Student Poster Symposium” from 11:00 AM-12:30 PM and “Poster Session A” from 3:30 PM-4:45 PM, on Sunday, June 25th.
Prior research on long COVID focuses on biological determinants; however, recent commentary suggests incorporating social and experiential factors into models of the disease may provide more explanatory power. We use the Household Pulse Survey–a survey administered collaboratively through multiple federal agencies–to help answer this question.
Authors: James Campbell (Presenter), Lynn A. Blewett, Robert Hest

