
Basics Blog
SHADAC has created a series of “Basics Blogs” to familiarize readers with common terms, concepts, and topics that are frequently covered. See all Basics Blogs here.
Executive Summary
- Countercyclical government policies and programs generally increase spending during economic downturns, and decrease spending during periods of economic growth.
- The Medicaid program operates as a countercyclical program to safeguard access to affordable health care coverage—a need that is reinforced during periods of economic contraction.
- Medicaid is jointly financed and operated by both the federal government and state governments, though the responsibilities are not divided 50-50.
- States carry the bulk of the responsibility for administering their Medicaid program.
- The federal government plays a smaller role, providing oversight and ensuring that states conform to federal laws and regulations.
- The federal Medicaid funding received by a state program varies depending on numerous factors, including the number of individuals using the state’s Medicaid program. The formula used to determine the federal government’s contribution to a state’s Medicaid program is called the Federal Medical Assistance Percentage—FMAP for short.
- State Medicaid programs have provided needed protection for individuals and/or families experiencing job loss or made newly-poor during unexpected economic downturns for decades, including during every recession over the past 25+ years.
Introduction
One of the features of the modern U.S. economy is the recurring fluctuation between economic growth and contraction, a pattern commonly called the “economic cycle.” While the economic cycle has broad implications for society overall, it also has important effects on individuals and families. When the economy enters a contraction phase and shrinks (i.e., a recession), businesses typically respond by cutting costs—which often entails eliminating jobs, trimming employees’ hours or rates of pay, and reducing benefits.1
Those kinds of cost reduction strategies can leave individuals and families in a bind: they need work and the money that comes from it, as well as the benefits that employers frequently provide (e.g., health insurance). In fact, the primary source of health insurance coverage for a majority of people living in the U.S. comes from an employer, called employer-sponsored insurance. But because so many businesses are usually seeking to reduce costs during a weak economy, it can be extremely difficult for people to find a replacement job when demand for jobs is high but supply is low.
That dilemma is why so many governments around the world have implemented countercyclical fiscal policy and operate countercyclical programs that help soften economic slumps – the Medicaid program being one example in the United States. But what exactly is a countercyclical policy or program? And how does this type of activity protect people during recessions?
In this blog, we define in plain language what a countercyclical program is and discuss the countercyclical aspects of Medicaid, a critical source of health insurance for millions of low-income individuals.
We begin with a general look at what we mean when we say a countercyclical policy or program. Then, we move into an overview of Medicaid funding, including how state Medicaid programs are financed and the role of the federal government in Medicaid funding followed by examples of how Medicaid performed when unemployment rates rose during the three most recent U.S. economic recessions.
What Does Countercyclical Mean? Countercyclical Policy & Program Definition
In the context of this blog, the term “countercyclical” refers to how government spending relates to the overall state of the economy, increasing during economic downturns and decreasing during periods of economic growth. Countercyclical spending runs counter to the actual state of the economy. In contrast, “procyclical” spending increases when the economy is growing. An example of procyclical government spending is that spending on K-12 education tends to increase during periods of economic growth, as tax revenues increase.

Countercyclical policy and government programs generally increase spending during periods of economic contraction. Rather than leaving individuals and families without the ability to afford even basic necessities during economic downturns, such as food, housing, and health care, the idea is that government programs step in to temporarily fill gaps while the economy recovers.
For instance, government unemployment insurance programs provide workers with cash when they have lost their jobs during a recession, and food assistance programs (e.g., the Supplemental Nutrition Assistance Program, SNAP) help make meals more affordable for families when the economy shrinks and their incomes are reduced.
Of course, these supports are available at all times, not just during economic downturns. So why would spending increase during recessions for these types of countercyclical programs?
During economic downturns, more people lose their jobs or experience reductions in hours worked, and more people need help paying for health care and other resources than during times of economic stability or growth. Thus, spending on these countercyclical programs increases during economic recession as more people need and are eligible for the assistance those programs provide—something that is done by design to address needs that are hard to predict.
Medicaid Is a Countercyclical Program
Like government unemployment insurance and SNAP, the Medicaid program is designed to be a countercyclical program that responds to the usual increase in the number of people that become eligible for benefits during economic downturns. As more individuals lose their jobs – and their employer-sponsored health coverage - or experience pay cuts, making them newly eligible for public health insurance coverage, many turn to Medicaid as a crucial health coverage backstop.
You can see in Exhibit 1 below (from a recent publication by the Medicaid and CHIP Payment and Access Commission (MACPAC)) how trends in unemployment rates and Medicaid enrollment corresponded during the Great Recession – as unemployment went up, so did Medicaid enrollment.
Exhibit 1. MACPAC, Unemployment Rate and Medicaid Enrollment During Great Recession
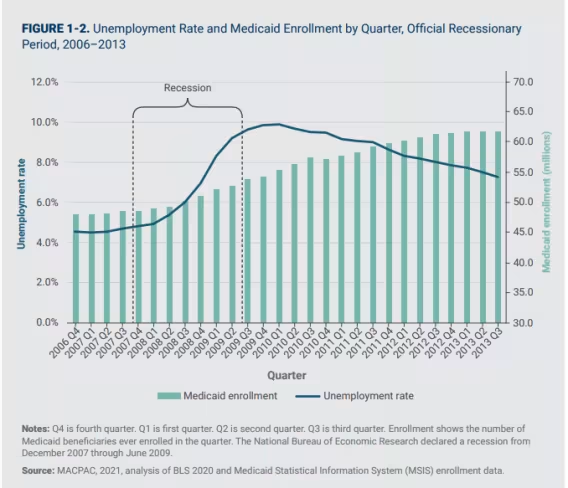
Source: Medicaid and CHIP Access and Payment Commission (MACPAC). (2020). Considerations for Countercyclical Financing Adjustments in Medicaid (pp. 1–24). https://www.macpac.gov/wp-content/uploads/2020/06/Considerations-for-Countercyclical-Financing-Adjustments-in-Medicaid.pdf
Medicaid Financing and Administration
So, we know that Medicaid is designed as a countercyclical program, with spending increasing during a weak economy. But how is Medicaid financed and administered, exactly?
Medicaid is jointly financed and operated by both the federal government and state governments, though the responsibilities are not divided 50-50. Instead, states carry the bulk of the responsibility for the administration of their respective Medicaid programs while the federal government plays a smaller role, providing oversight and ensuring that states conform to federal laws and guidance.
For example, states design how they want their Medicaid program to run: they name their programs (which is why the names vary across the states), set eligibility standards such as income thresholds (i.e., who qualifies for Medicaid, based on “low income”), and decide which health care services are covered by their Medicaid program.
States also hold responsibility for administering their Medicaid programs, including processes for enrolling people who apply and are found eligible for coverage, renewing coverage, and disenrolling people who no longer qualify for coverage, such as if their income increases. States are also responsible for processing and paying health care providers for services provided to Medicaid enrollees (though many states delegate this responsibility to third-party contractors, including Medicaid managed care organizations).
As you can see, states take on a majority of the responsibilities for the design and implementation of their Medicaid programs compared to the federal government.
However, the federal and state roles for funding Medicaid are flipped, with the federal government generally paying a larger share of Medicaid costs and states paying a smaller share. The precise amount of federal funding that states receive for their Medicaid programs varies based on a variety of factors determined by federal law.
Federal Contribution to Medicaid Funding
The federal Medicaid funding received by a state program varies depending on numerous factors, including the number of individuals using the state’s Medicaid program. The formula used to determine the federal government’s contribution to a state’s Medicaid expenditures is formally called the Federal Medical Assistance Percentage—FMAP for short.
In general, a state’s FMAP varies based on its average income compared to the U.S. average income. The federal government pays a higher share of Medicaid spending for lower-income states than it does for higher-income states. (See Exhibit 2 for the FMAP percentages by state and territory.)2
Exhibit 2. FMAP Percentages by Geography, Fiscal Year 2025
| FMAP Percentage | Number of States | States |
|---|---|---|
| Minimum: 50.00% | 10 | CA, CO, CT, MD, MA, NH, NJ, NY, WA, WY |
| 50.01-55% | 6 | AK, IL, MN, ND, SD, VA |
| 55.01-60% | 8 | FL, HI, NE, OR, PA, RI, TX, VT |
| 60.01-65% | 12 | AZ, DE, IN, IA, KS, ME, MT, NV, OH, TN, UT, WI |
| 65.01-70% | 9 | DC, GA, ID, LA, MI, MO, NC, OK, SC |
| 70.01-75% | 5 | AL, AR, KY, NM, WV |
| 75.01-80% | 2 | MS, PR |
| Maximum: 83.00% | 4 | AS, GU, MP, VI |
Source: SHADAC synthesis of Medicaid and CHIP Payment and Access Commission (MACPAC). (2024). MACStats: Medicaid and CHIP Data Book (pp. 1–157). https://www.macpac.gov/wp-content/uploads/2024/12/MACSTATS_Dec2024_WEB-508.pdf
Since the beginning, the Medicaid program was designed so that federal spending increases along with state spending, without a cap in federal spending.3 This design is especially relevant during economic downturns, because state Medicaid program spending tends to increase quickly (as more people become eligible for the program as they lose work)—thus, federal spending automatically increases during these times in proportions established by FMAP rates.
State Contribution to Medicaid Funding
States fund their share of Medicaid expenditures in a variety of ways, including general income and sales tax (General Fund Revenue), special taxes collected from health care providers, and other state and local financing mechanisms.4
However, states face a critical challenge during recessions. At precisely the time their Medicaid costs are increasing, largely due to increasing enrollment as workers lose their jobs or face pay cuts, the recession is simultaneously reducing their tax revenues.5
(Exhibit 3 below shows the trends in state tax revenue growth during recessions, where you can clearly see reduced tax revenue during economic downturns, such as the Great Recession between 2007 and 2009).
Exhibit 3. State Tax Revenue Annual Growth Rates and Recent Recessions (2000 – 2020)
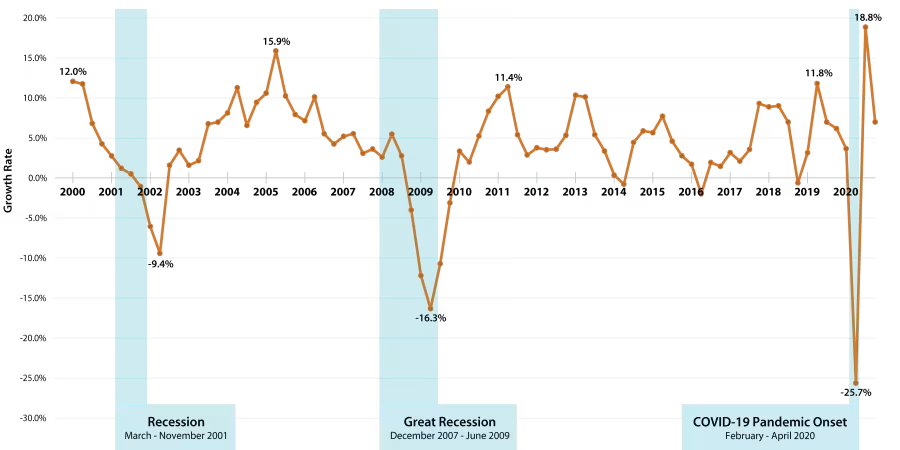
Source: SHADAC Analysis of U.S. Census Bureau, Quarterly Summary of State and Local Tax Revenue, Table 3. Adapted from Snyder, L., & Rudowitz, R. (2016, June 21). Trends in State Medicaid Programs: Looking Back and Looking Ahead. KFF. https://www.kff.org/medicaid/issue-brief/trends-in-state-medicaid-programs-looking-back-and-looking-ahead/view/print/
But most states are required to balance their budgets, meaning their total revenues need to match or exceed their total expenses. They are unable to operate with less funding than is needed to cover expenditures in a given year, which is known as a budget deficit or shortfall.
And, they are unable to carry over a budget deficit into a future year. So simply running a budget deficit or borrowing money during a recession is not an option for resolving the problem of reduced revenue.
Fiscal Stimulus During a Recession
We just went over how increased state spending also results in increased (and uncapped) federal spending for financing Medicaid – so why can’t the federal government just entirely make up for states’ reduced revenues during recession? While it’s true that the federal government is available to finance much of the increased Medicaid costs we tend to see during recessions (in line with FMAP standards), there are also guidelines that federal spending does not apply unless states also cover their share of Medicaid expenditures.
All of the factors we’ve gone over so far create uncertainty for many states during recessions. Because residents are losing income and jobs, state Medicaid programs see increased enrollment and costs. But, as state tax revenues usually decline during recessions, states also tend to have fewer dollars to devote to their Medicaid programs at the very same time their Medicaid program costs are increasing.
This often leads states to look for cost savings in their Medicaid programs. States could also consider freeing up more money to pay for growing Medicaid costs by cutting other important public spending, such as on education or infrastructure like roads and bridges.
Options for states to reduce Medicaid spending are seldom without their own pain. For instance, states may:
- Make changes to who is allowed to enroll in Medicaid, which could decrease the number of people who qualify for coverage;
- Reduce Medicaid offerings and benefits, which could leave some enrollees unable to afford or obtain some kinds of care;
- Reduce the how much Medicaid pays—or reimburses—hospitals, clinics, and other health care providers, which could harm the bottom-line of some health care providers or perhaps cause some health care providers to stop accepting patients with Medicaid coverage.
Simultaneously, reducing state spending on Medicaid automatically reduces federal spending, meaning that by reducing Medicaid expenditures, the state is effectively declining federal funds that could support the state economy.
Past recessions have revealed that even with the federal government promising to cover the majority of state Medicaid spending as programs grow and costs increase, the reduction in state tax revenues combined with increased state Medicaid costs placed unsustainable pressure on state budgets. For that reason, Congress has intervened by enacting temporary FMAP increases as part of broader federal economic relief packages during each of the three recessions of the past 25 years.
Image text: “Because the FMAP is already in place and can be quickly distributed, …. it is a mechanism the federal government can easily use to increase aid to states.” - NBER 20236
Countercyclical Policy and Medicaid Protections in Action During Recessions
State Medicaid programs have provided needed protection for individuals and/or families experiencing job loss or made newly-poor during unexpected economic downturns for decades. In order to demonstrate the beneficial effects of Medicaid’s countercyclical nature during recessionary periods, SHADAC reviewed selected research literature that discussed both Medicaid enrollment and one measure of economic activity: unemployment.7 (See SHADAC’s blog on trends for national and state-specific data on unemployment rates since the COVID-19 pandemic.)
While every recession is unique and the effects on state public health insurance coverage depend on a variety of factors, literature supports the concept that Medicaid provides a stabilizing role in ensuring access to coverage and health care at times when the U.S. economy falters.
Let’s take a look at the examples SHADAC researchers found during our scan of relevant literature:
2001 Recession
In 2001, the U.S. economy experienced a relatively short recession of less than a year, though some economic indicators (e.g., unemployment) took years to recover their lost ground. During this first economic downturn of the new millennium, unemployment increased, health insurance costs rose, and some small businesses stopped offering health insurance benefits to their employees.8
As we would expect, like unemployment rates, the percentages of those covered by Medicaid rose during this recession. One study using data from the National Health Interview Survey for 2002 and the first quarter of 2003 estimated that the percentage of children covered by Medicaid, “…rose from 23.6%in 2001 to 27.1% in 2002. The percentage of non-elderly adults covered rose from 9.4% to 10.3%.”9
By mid-2003, Congress passed federal fiscal relief, which included an FMAP increase to cover Medicaid spending shortfalls as program enrollment remained higher than before the 2001 recession.
The Great Recession, 2007 - 2009
During the Great Recession that began in 2007, unemployment doubled (and remained stubbornly high for years), and the number of adults without insurance increased along with the number of individuals and families enrolled in Medicaid.
A study by Holahan and Garrett relying on Current Population Survey (CPS) data (among other sources) estimated that an increase in unemployment was associated with decreases in employer-sponsored insurance as well as increases in Medicaid/CHIP coverage and uninsurance. Increases in Medicaid/CHIP coverage were larger for children than for adults.10
A study from Benitez et. al. used CPS data (and other sources) through 2011, estimating that states with more generous Medicaid eligibility guidelines were more likely than states with less generous eligibility to absorb the coverage losses caused by the recession (i.e., they experienced smaller increases in uninsurance).11,12
During this recession period, federal relief passed by Congress (American Recovery and Reinvestment Act) included a retroactive enhanced FMAP (conditional on maintaining certain eligibility policies), including additional support for states with high unemployment.
2020 Recession
The recession that ensued during the COVID-19 pandemic presented differently from the past two recessions. While unemployment and Medicaid enrollment both rose sharply, job losses were not consistently associated with state Medicaid enrollment growth.13,14
Additionally, unemployment rates began to decline quickly after the short recession (February to April 2020) ended. Congress also passed a continuous enrollment provision, such that state Medicaid programs were prohibited from disenrolling individuals until the public health emergency ended.
This was the first recession since the passage of the Affordable Care Act, which expanded Medicaid eligibility to newly eligible adults (e.g., adults with incomes up to 138% of federal poverty guidelines (FPG)). Benitez et. al. found a relationship between state Medicaid expansion status (i.e., whether states had accepted the ACA option to expand their Medicaid programs) and whether Medicaid enrollment increased at the same time unemployment increased.
Using CPS data to compare changes in Medicaid coverage among certain workers who lost their jobs in 2020 versus workers who remained employed, the authors estimated that Medicaid enrollment increased in both Medicaid expansion and non-expansion states—but the size of the increase was larger in Medicaid expansion states.15
In part because the pandemic crisis was deeply intertwined with the health care sector, Congress acted quickly to provide fiscal relief to state Medicaid programs who were seeing rising enrollment and spending. All states took advantage of the option to receive an enhanced FMAP (under the Families First Coronavirus Response Act) contingent on not limiting program eligibility or affordability.
Medicaid and Countercyclical Policy Protect Access to Health Care Coverage
The U.S. Medicaid program operates as a countercyclical program for ensuring people have affordable access to health care coverage—a need that is reinforced during period of economic contraction, when many individuals and families face job loss and reduced income.
As you could see from the examples above from the three most recent recessions, despite their differences, increased spending & protections for eligibility and coverage were shared similarities. In each of these recessions, we saw the economy constricted (with increased unemployment), increased enrollment in Medicaid, and federal intervention & increased Medicaid spending - all factors aligning with Medicaid’s countercyclical design, and supporting that design protects Americans’ health care during recession.
Due in part to Medicaid’s countercyclical financing, in which government spending increases when the economy contracts, state Medicaid programs serve as safeguards when access to affordable health insurance coverage and care are at greatest risk.
However, the complex structure of the program also poses challenges to the ability for Medicaid to fully meet the growing need when the economy slows. Over the past 25 years, interventions by Congress in times of economic downturns have helped Medicaid to weather those inherent challenges, increasing federal matching funds as a way to lighten the pressure on state budgets.
That has allowed Medicaid to more effectively serve its countercyclical purpose of ensuring that people don’t lose health insurance and access to health care when the economy contracts. Research on the role Medicaid has played in protecting people’s access to health care during the recent recessions has affirmed the idea that the program provides an important backstop during recessions, as you could see just from SHADAC’s scan of literature above.
State Medicaid expenditures vary depending on the economy as well as state decisions regarding program eligibility, coverage, and reimbursement. Countercyclical fiscal policy, both by design and through federal intervention, allows state Medicaid programs to continue to provide the social protection people needed during unexpected downturns in the economy.
To learn more about health care access and stay up-to-date on the latest in Medicaid policy, we encourage you to sign up for SHADAC’s monthly newsletter. You’ll get our latest articles, updates, and resources sent straight to your inbox. Sign up here!
Notes
1 The National Bureau of Economic Research (NBER) identifies and tracks changes in U.S. economic activity.
2 The Children’s Health Insurance Program (CHIP) and the ACA Medicaid expansion population are financed at higher FMAP rates.
3 Although, one important exception to this is how Medicaid operates in the U.S. territories (e.g., American Samoa, the Commonwealth of the Northern Mariana Islands, Guam, Puerto Rico, and the U.S. Virgin Islands), in which federal Medicaid spending has an annual cap, and where FMAP formulas governing the federal share of spending do not apply in the same way as in the states.
4 Blewett, L. A. (2021, March 24). New State Health Compare Measure: Medicaid Expenses as a Percent of State Budgets. State Health Access Data Assistance Center (SHADAC). https://www.shadac.org/news/new-state-health-compare-measure-medicaid-expenses-percent-state-budgets
5 Allen, H. L., & Sommers, B. D. (2020). Medicaid and COVID-19. JAMA, 324(2), 135–136. https://doi.org/10.1001/jama.2020.10553
6 Dague, L., & Ukert, B. D. (2023, June 1). Pandemic-Era Changes to Medicaid Enrollment and Funding: Implications for Future Policy and Research. National Bureau of Economic Research. https://doi.org/10.3386/w31342
7 Other measures of economic activity include, but are not limited to, gross domestic product and personal income.
8 Ku, L. (2003, September 23). CDC Data Show Medicaid and SCHIP Played A Critical Counter-Cyclical, Revised 10/8/03. Center on Budget and Policy Priorities. https://www.cbpp.org/sites/default/files/archive/9-23-03health.htm
9 Ibid.
10 Holahan, J., Garrett, A. B., & The Urban Institute. (2009). Kaiser Commission: Rising Unemployment, Medicaid and the Uninsured (pp. 1–14). The Henry J. Kaiser Family Foundation. https://www.kff.org/wp-content/uploads/2013/03/7850.pdf
11 Authors categorized states using a generosity index, defined as “…the share of a common, nationally representative sample of nonelderly and nondisabled adults that would be eligible for Medicaid under each state’s 2007 guidelines.” For more details, see footnote 12.
12 Benitez, J., Perez, V., & Seiber, E. (2020). Medicaid Access During Economic Distress: Lessons Learned From the Great Recession. Medical Care Research and Review, 78(5), 107755872090923. https://doi.org/10.1177/1077558720909237
13 Frenier, C., Nikpay, S. S., & Golberstein, E. (2020). COVID-19 Has Increased Medicaid Enrollment, But Short-Term Enrollment Changes Are Unrelated To Job Losses. Health Affairs, 10, 10.1377/hlthaff. https://doi.org/10.1377/hlthaff.2020.00900
14 Khorrami, P., & Sommers, B. D. (2021). Changes in US Medicaid Enrollment During the COVID-19 Pandemic. JAMA Network Open, 4(5), e219463. https://doi.org/10.1001/jamanetworkopen.2021.9463
15 Non-expansion states included AL, FL, GA, KS, MS, MO, NE, NC, OK, SC, SD, TN, TX, WI, WY. Benitez, J., Williams, E., & Rudowitz, R. (2022, December 13). Medicaid Enrollment among the Unemployed During the COVID-19 Pandemic and Beyond. KFF. https://www.kff.org/medicaid/issue-brief/medicaid-enrollment-among-the-unemployed-during-the-covid-19-pandemic-and-beyond/