
Basics Blog
SHADAC has created a series of “Basics Blogs” to familiarize readers with common terms, concepts, and topics that are frequently covered. See all Basics Blogs here.
This Basics Blog will focus on the concept of health equity. We will answer and provide explanations for questions like:
- What is health equity?
- What is the definition of health equity?
- How can we talk about health equity in public health work?
- What are other supplemental terms and their definitions that are used in the health equity space?
With that foundation set, we then move into an example, using a study on provider discrimination data drawn from the Minnesota Health Access Survey (MNHA) to understand how to apply a health equity lens to public health work and analysis. Finally, we end with some further thoughts and considerations on our evolving understand of this complex concept.
Keep on reading below to learn more about health equity.
Health Equity Definitions
The Robert Wood Johnson Foundation, a philanthropic organization dedicated to advancing health equity and dismantling barriers in health care, defines health equity below:
It is important to note, though, that since health equity is conceptual, there is not a singular definition of it. This definition can also change and evolve, so it’s important to continue to educate yourself on health equity as time goes on.
What Is the Difference Between Equity and Equality?
While these two concepts are similar, equity and equality are not one in the same.
Equality is defined as giving the same treatment to everyone, regardless of individual needs or differences.
Equity is defined as giving treatment that is specific to individual needs, which allows everyone a fair chance at being successful.
The graphic below from the Robert Wood Johnson Foundation provides a visual representation of the difference between equality and equity. In the ‘Equality’ example, all people are given the same mode of transportation – they are given equal treatment. However, because the individual’s needs are not considered, the outcome is not necessarily equal as can be seen in the visual. In the ‘Equity’ example, each individual is given a mode of transportation that works for their needs, leading to a more equitable outcome as can be seen in the example.
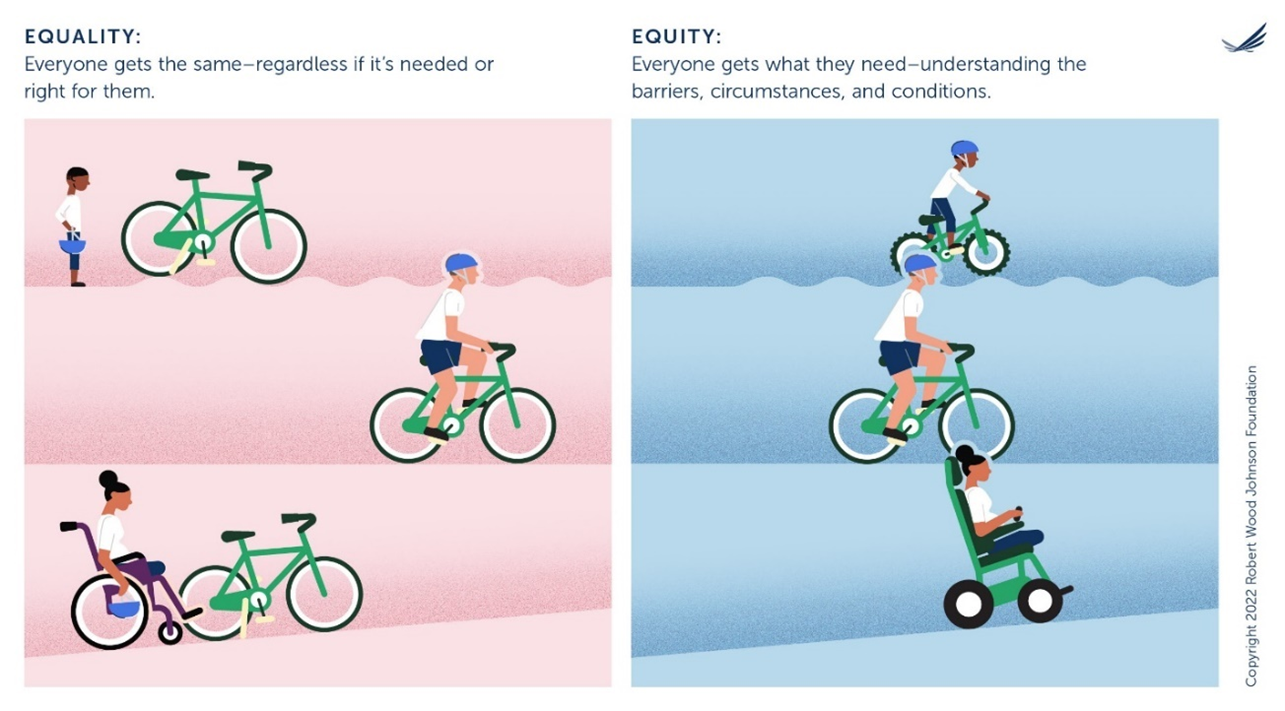
Source: Joan Barlow, “We Used Your Insights to Update Our Graphic on Equity” Robert Wood Johnson Foundation, November 2022, We Used Your Insights to Update Our Graphic on Equity (rwjf.org). Reproduced with permission of the Robert Wood Johnson Foundation, Princeton, N.J.
Additional Terminology Definitions
The topic of health equity is complex, with many factors feeding into it. To further understand health equity, it is important to define these additional factors and terms as well. While this list is not exhaustive, the terms below all refer to larger barriers and systems that must be addressed in order to reach equity in health and health care.
Health Disparities: Avoidable differences in health outcomes experienced by people with one characteristic (race, gender, sexual orientation, etc.) as compared to the socially dominant group (e.g., white, male, cis-gender, heterosexual, etc.).
Measuring disparities can benchmark progress toward achieving health equity.
Social Determinants of Health (SDOH): The daily context in which people live, work, play, pray, and age that affect health. SDOH encompass multiple levels of experience from social risk factors (such as socioeconomic status, education, and employment) to structural and environmental factors (such as structural racism and poverty created by economic, political, and social policies).
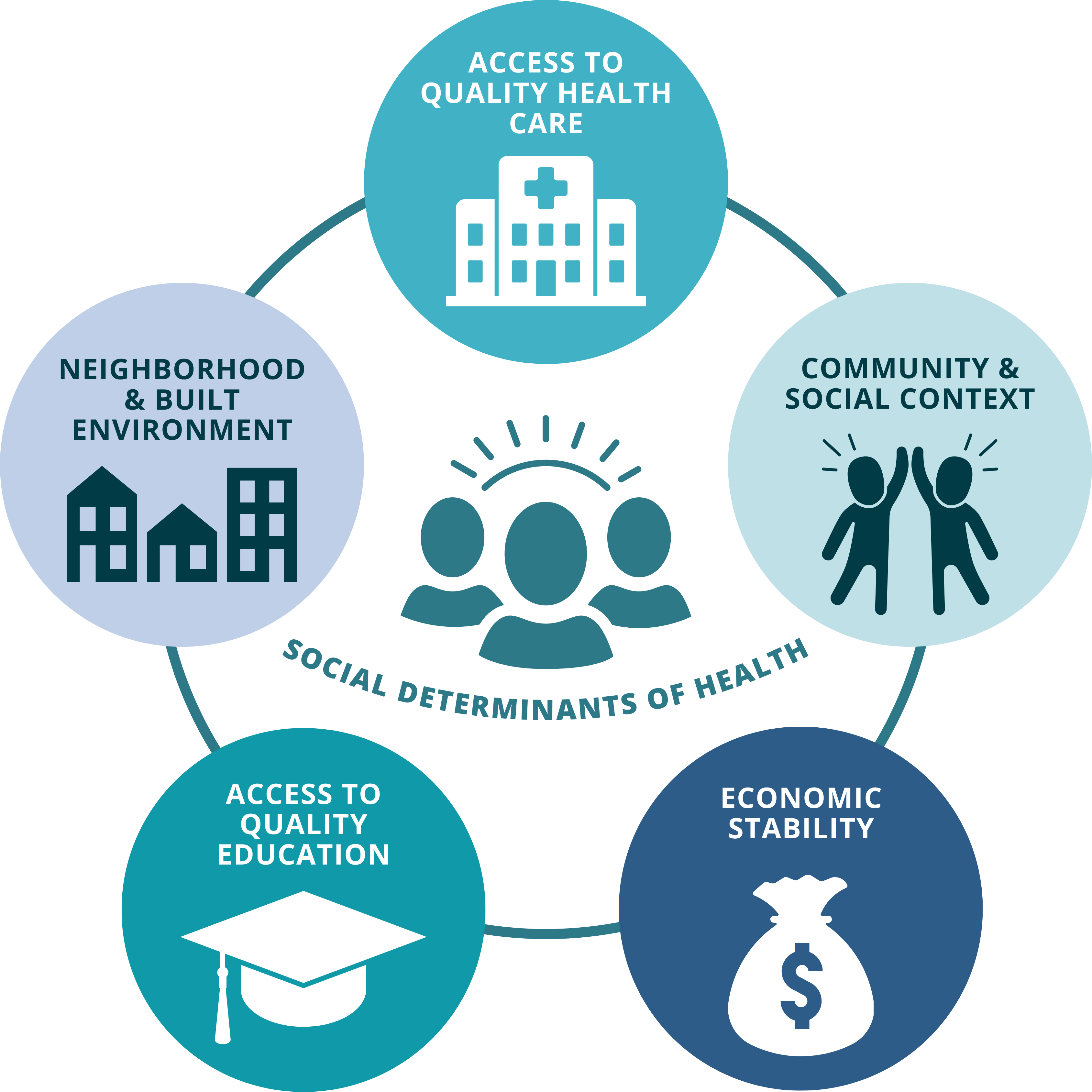
These factors are known quantities that contribute to social and health inequities.
Social Inequities: Differences between groups that are unfair, unjust, systemic, and avoidable. Social inequities can be characterized by race, ethnicity, gender, age, sexual orientation, income, etc.
Social inequities can lead to poor health outcomes and further perpetuate systems and circumstances leading to health disparities (systemic racism, ableism, etc.).
Structural Racism: A complex system rooted in historical and current realities of differential access to power and opportunity for different racial groups. This system is embedded within and across laws, structures, and institutions in a society or organization. This includes laws, inherited disadvantages (e.g., the intergenerational impact of trauma) and advantages (e.g., intergenerational transfers of wealth), and standards and norms rooted in racism.
Structural racism contributes to a number of social determinants of health (SDOH). Public health systems must prioritize addressing structural racism as a primary barrier to health equity.
As you can see, many of these terms contribute to each other or are a result of another—truly showing how complex the topic of health equity is.
Using a Health Equity Lens on Provider Discrimination—Challenges and Interventions
Now that we have gone over some helpful terminology to keep in mind, let’s look at how to apply a health equity lens when looking at a real-life public health example.
The example we will go over in this section is related to LGBTQ+ health equity and discrimination. With roughly 13.9 million adults in the United States identifying as LGBTQ+, this example is both relevant and important for conversations on equity. Individuals of minoritized sexual orientation and gender identity have been historically marginalized, underrepresented in data, and faced with many health disparities, compared to their heterosexual, cisgender counterparts. These disparities exist for LGBTQ+ people not only at the national level, but also at the community, organizational, and smaller societal levels.
Thus, in June 2022, President Biden signed Executive Order 14075: Advancing Equality for Lesbian, Gay, Bisexual, Transgender, Queer, and Intersex Individuals. This executive order is a sign of progress toward breaking down systemic barriers and more relatedly for this blog, empowering the Secretary of Health and Human Services (HHS) to “promote the adoption of promising policies and practices to support health equity” for this population.
Now we will look specifically at a relevant measure from the Minnesota Health Access Survey (MNHA) – provider discrimination by sexual orientation and gender identity (SOGI) in Minnesota – to demonstrate how we can perform studies, analyze results, and identify accessible solutions to health disparities by viewing them through a health equity lens.
The Data
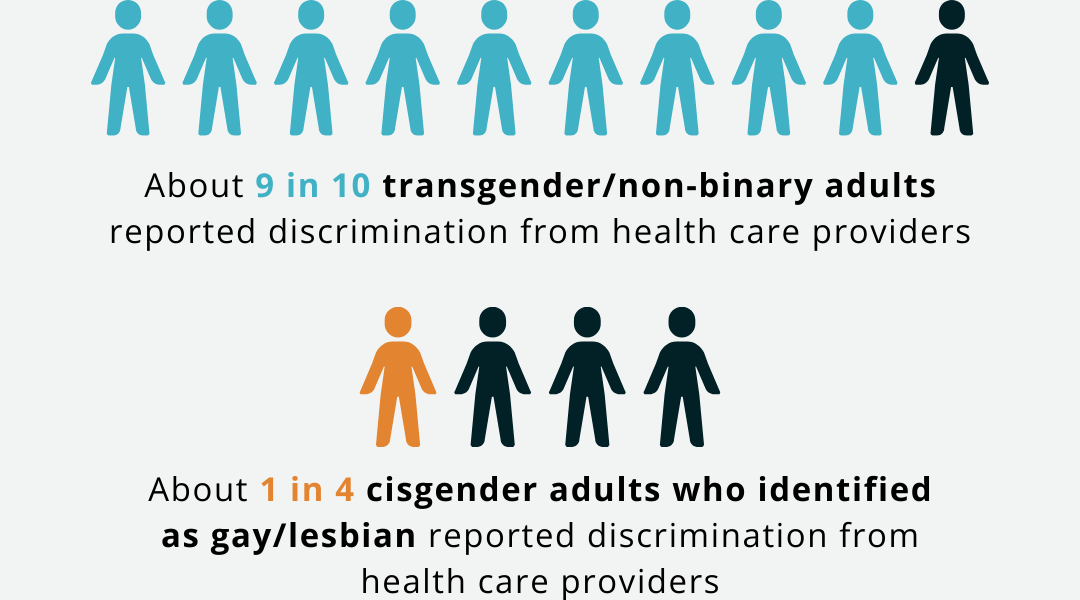
Data coming from the 2021-2023 Minnesota Health Access Survey (MNHA) reveals that among all adults in Minnesota, over half of the transgender/non-binary population (56.3%) reported experiencing Sexual Orientation and/or Gender Identity (SOGI) based discrimination from health care providers – significantly higher compared with cisgender adults’ reported experiences of discrimination (6.7%).
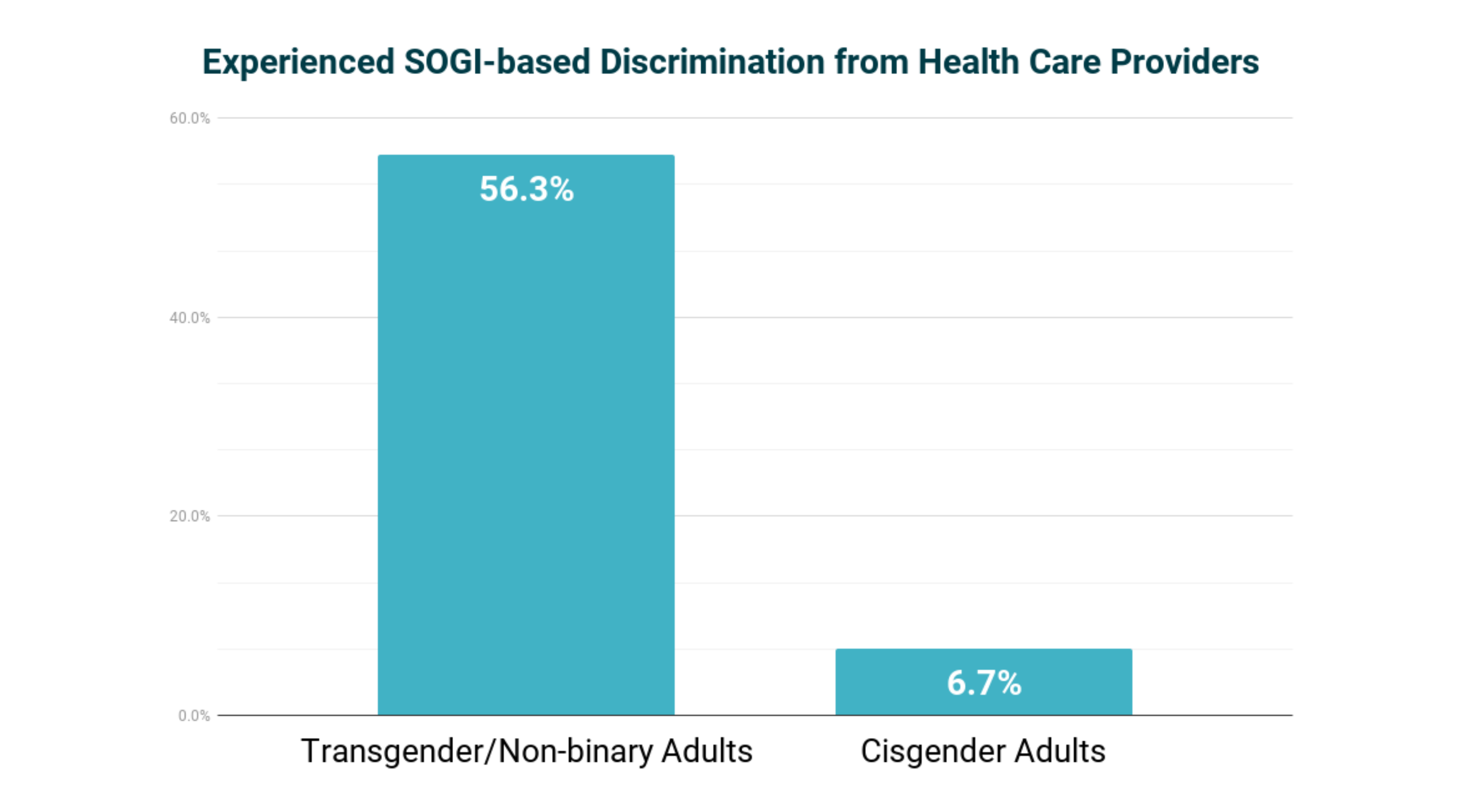
Nearly 9 in 10 transgender/non-binary adults (88.1%) and about one in four (24.1%) cisgender adults who identified as gay/lesbian reported discrimination. Two thirds of transgender/non-binary adults (66.1%) and about a quarter of cisgender adults (23.9%) that chose the ‘none of these’ option for sexual orientation also reported discrimination. Discrimination among people who identify as bisexual/pansexual is also high, and not statistically different for transgender/non-binary adults (40.5%) and cisgender adults (31.6%).
Experiencing discrimination has been shown to negatively affect both mental and physical health, as individuals and members of historically marginalized communities report worse health status and may forgo or delay care to avoid further discrimination.
Now, let’s look at potential ways to equitably address instances of provider discrimination by sexual orientation and gender identity at various levels.
Community Level
There are various ways to approach the issue of addressing provider discrimination. One potential solution is to make changes to education for the overall medical community, such as implementing cultural competency and communication training.
Cultural competency describes services, practices, and processes that are responsive to diverse practices, assets, needs, beliefs, and languages for an array of individuals and communities. Examples of incorporating cultural competence in health care include:
- Promoting awareness and knowledge
- Recognizing one’s biases
- Engaging in cultural competence & bias training
- Using accessible language
- Familiarizing oneself with the local community
- Recruiting diverse team members
Embracing these strategies can help immensely in understanding and reducing stigma as well as strengthening relationships between providers and the unique communities they serve.
Incorporating cultural competence into care can therefore offer meaningful ways to make strides toward reducing reported discrimination rates, such as those from individuals reporting SOGI-based provider discrimination in Minnesota. When cultural competence is practiced, better and more equitable health outcomes are observed for patients. Improved trust and communication between providers and patients can lead to more regular interactions with the health care system (like routine preventative visits), which can in turn lead to better treatments, health outcomes, and even better overall health status, another known issue for LGBTQ+ individuals.
Organizational Level
Addressing provider discrimination at a higher organizational level can be done through changing health systems and how they operate. Structural issues, such as payment/reimbursement structures, lack of time for visits, and workforce diversity may also contribute to the discrimination felt by different individuals.
Structural competency, which is the belief that inequalities in health must be conceptualized in relation to the institutions and social conditions that determine health related resources, can then play a crucial role in promoting equitable care alongside cultural competency by addressing issues at a structural level. This concept can be implemented in health systems through training in five core competencies:
- Recognizing the structures that shape clinical interactions
- Developing an extra-clinical language of structure
- Rearticulating “cultural” formations in structural terms
- Observing and imagining structural interventions
- Developing structural humility
Structural training and education helps medical professionals more effectively understand the economic and social determinants of health (SDOH) that occur for their patients before any interaction with the health care system occurs. In the instance of individuals belonging to the LGBTQ+ community, these can take the shape of lack of health insurance coverage or access barriers. Additionally, organizations can invest in structural changes to advance health equity through improved data systems that are able to track populations’ diverse makeup (race, ethnicity, sexual orientation, gender identity, primary language), alongside SDOH (income, education, employment) and health needs (utilization of care, treatment, and health outcomes), to better understand who they are serving and how to improve services.
Societal Level
On a larger scale, the state of Minnesota has made it a goal to ensure all Minnesotans receive high quality health care, free of provider or system bias.
Citing the 2021 Minnesota Health Access Survey (MNHA) data on responses to unfair treatment, the Minnesota Department of Health (DHS) recognized the disparity between the higher rates of unfair treatment by Black Minnesotans (39%) and Transgender Minnesotans (50%) compared to White Minnesotans and cis-gendered men (9% and 12%, respectively), and created a measurable goal to directly address this issue.
By 2027, MN DHS states that it hopes to reduce the percentage of transgender and non-binary Minnesotans and Black Minnesotans reporting unfair treatment by their providers by 50%. This goal is a meaningful step toward health equity for individuals with different racial and ethnic backgrounds and different gender identities.
Shifting Definitions and Future Considerations
In the example above, examining reported rates of provider discrimination in Minnesota and potential solutions at different levels helps to understand not only a practical example of how better understanding of health equity and systemic issues can clarify what the major barriers to advancing equity look like, but also how they can be addressed.
Even now as the definition of health equity is not set in stone and continues to evolve, we see opportunity for solutions to advance health equity--both in general, and for people with minoritized sexual and gender identities--to evolve as well. However, this does not apply only to health equity, as the definitions and understanding of many of the terms described above have evolved over time. As society and demographics continue to shift, so does our insight and understanding of these concepts.
There is a need for more involvement at the community, organizational, and societal level in advancing health equity. While there is progress in the right direction, there are still structural barriers that need to be overcome and met with applicable solutions that lead to positive systemic change.
Interested in learning more about health equity? Now that you have the SHADAC Basics down, try some of the following resources to continue to expand your knowledge: