
Blog & News





Studying the Impact of COVID-19: State-Level Data Resources on State Health Compare
April 20, 2020:Though the spread of disease caused by the novel coronavirus (COVID-19) has impacted the lives of individuals across the United States, the magnitude of the virus' effects has varied greatly across different states. Access to current, accurate state-level data is important in order to inform state researchers, analysts, and policymakers’ efforts to understand and respond to the disparate impacts of COVID-19 on their resident populations.
To that end, this blog provides a high-level overview of a range of data measures currently housed in our online data tool, State Health Compare, as well as a number of related resources that provide more in-depth analysis for certain measures. Notably, estimates for each of the measures listed are available for subpopulations that often highlight persistent disparities in health—a feature that may prove especially useful as calls to further break down data related to COVID-19 into subcategories (e.g., gender, age, race/ethnicity, etc.) to track the impact of the disease on specific populations have recently increased.
Risk Factors
Chronic Disease Prevalence
This measure captures the percent of adults who reported having one or more common chronic conditions such as diabetes, cardiovascular disease, heart attack, stroke, or asthma. It includes breakdowns by race/ethnicity and educational attainment. (2005-2010, 2011-2019)*
Adult Smoking
This measure shows the percent of adults who reported smoking, defined as adults who have smoked 100 or more cigarettes in their lifetime and who currently smoke some days or every day. The measure is broken down by race/ethnicity and educational attainment. (2005-2010, 2011-2019)*
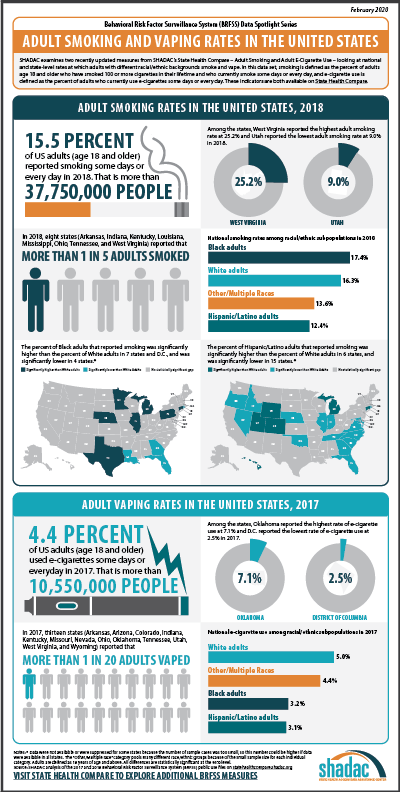
Related Resource: SHADAC researchers used data from the Behavioral Risk Factor Surveillance System (BRFSS) to produce analyses focused on several different health behaviors, including Adult Smoking and E-cigarette Use in the United States. This blog, part of a spotlight series including binge drinking and obesity, looks at national and state-level rates at which adults with different racial/ethnic backgrounds smoke and vape in 2018 and 2017.
State Health Funding
Medicaid Expenses as Percent of State Budget
This measure captures state and federal spending on Medicaid as a share of each state’s budget. (2000-2018)
Public Health Funding
This measure shows state public health funding per capita by fiscal year. (2005-2019; no data available for 2006)
Related Resource: SHADAC researchers produce an annual brief, Exploring Public Health Indicators with State Health Compare: State Public Health Funding, exploring the wide variation in per capita public health funding by state, and why public health funding data, in conjunction with state performance on other public health indicators, might signal which states are best suited to absorb a potential decrease in funding and which states might be hit hardest.
Access to Health Care
Had Usual Source of Medical Care
This measure counts the percent of people who had a usual source of medical care other than the emergency department (i.e., doctor’s office, clinic, health center, etc.) in the past year. Breakdowns by age and coverage type are also available. (2011-2017)
Adults with No Personal Doctor
This measure denotes the percent of adults without a personal doctor and offers breakdowns by education level and race/ethnicity. (2005-2010, 2011-2019)*
Related Resource: SHADAC recently produced a blog and infographic - Affordability and Access to Care in 2018: Examining Racial and Educational Inequities across the United States (Infographic) - focusing on racial/education inequities in access and ability to afford medical care, using this measure along with estimates for Adults Who Forgo Needed Medical Care.
Broadband Internet Access
This measure shows the percent of households that have a broadband internet subscription (i.e., that pay a cell phone or internet services provider for the service), which includes a cellular data plan, cable, fiber optic, DSL, or satellite internet service. (2016-2018)
Related Resource: A new SHADAC blog explores the way that Internet Access Measures the Impact of the Digital Divide and COVID-19. An initial analysis of the estimates shows variation in access to broadband across states, and reveals disparities by income, rurality, coverage, and disability status.
Insurance Coverage
Coverage Type
This measure shows the rates of different types of health insurance coverage, including Medicare, employer-sponsored insurance (ESI), Medicaid, and individual coverage, as well as no insurance coverage. Users can view this measure by a variety of breakdowns, including: age, citizenship, disability status, education, family income, health status, limited English proficiency, marital status, poverty level, race/ethnicity, sex, and work status. (2008-2018)
Health Care Costs and Affordability
People with High Medical Care Cost Burden
This measure highlights the percent of individuals in families where out-of-pocket health care spending, including premiums, has exceeded 10 percent of annual income. Breakdowns by employer coverage, income, and race/ethnicity are available for each state. (2010-2012, 2013-2017, 2017-2018)*
Medical Out-of-Pocket Spending
This measure estimates the annual median family “out-of-pocket” spending, including premiums, on health care costs that are typically not covered by health insurance but paid for out of an individual’s own resources. These costs can include copays for doctor and dentist visits, diagnostic tests, prescription medicine, glasses and contacts, and medical supplies. (2017-2018)
Related Resource: SHADAC used this measure to produce a brief entitled State-level Estimates of Medical Out-of-Pocket Spending for Individuals with Employer-sponsored Insurance Coverage, which shows state variation in medical out-of-pocket spending (with a brief section that also looks at high medical cost burden) for people with employer-sponsored insurance.
High-Deductible Health Plans
This measure reports the percent of private-sector employees enrolled in high-deductible health insurance plans. High-deductible health plans are defined as plans that meet the minimum deductible amount required for Health Savings Account (HSA) eligibility (e.g., $1,350 for an individual and $2,700 for a family in 2018); breakdowns by firm size are offered. (2012-2019)
Average Annual ESI Deductible and Average Annual ESI Premium
This first measure reports the average annual deductible for private-sector workers who receive a health insurance plan through their employer that has a deductible. The second measure reports the average annual premium for private-sector workers who get health insurance through their employer. Both measures can be broken down by plan type (family or single). (2003-2019; partial data for 2002)
Related Resources: SHADAC produces an annual report, the latest being State-level Trends in Employer-sponsored Insurance (ESI), 2014-2018, focused on the more than 62 million private-sector employees enrolled in Employer-Sponsored Insurance (ESI) coverage and their growing out-of-pocket costs. The report includes a narrative summary, interactive map, two-page state profiles, and data tables.
From the data used to produce our annual ESI report, SHADAC researchers also created A Deeper Dive on Employer-sponsored Health Insurance: Costs in Five States in Comparison with the United States; a focused, five state analysis of ESI trends in order to better understand which states are most affected by increasing premiums and deductibles or might have a population with high enrollment in high-deductible health plans (HDHPs), leaving them financially vulnerable in case of an unexpected health crisis that leads to large medical bills.
Adults Who Forgo Needed Medical Care
The measure indicates the percent of adults in each state who could not get needed medical care due to cost. Breakdowns by education level and race/ethnicity are available for all states. (2005-2010, 2011-2019)
Related Resource: SHADAC recently produced a blog and infographic - Affordability and Access to Care in 2018: Examining Racial and Educational Inequities across the United States (Infographic) - focusing on racial/education inequities in access and ability to afford medical care, using this measure along with estimates for Adults with No Personal Doctor.
Trouble Paying Medical Bills
This measure tracks the rates of individuals who had difficulty paying off medical bills during the past twelve months or that were paying off medical bills over time. The measure can be broken down by age and insurance coverage type. (2011-2017)
Related Resource: In light of rising health care cost burdens, SHADAC produced a blog, Measuring Health Care Affordability with State Health Compare: Trouble Paying Medical Bills, assessing changes and patterns in health care affordability across the United States by tracking the percent of individuals that had difficulty paying off medical bills currently or over time.
Explore these measures on State Health Compare!
Notes
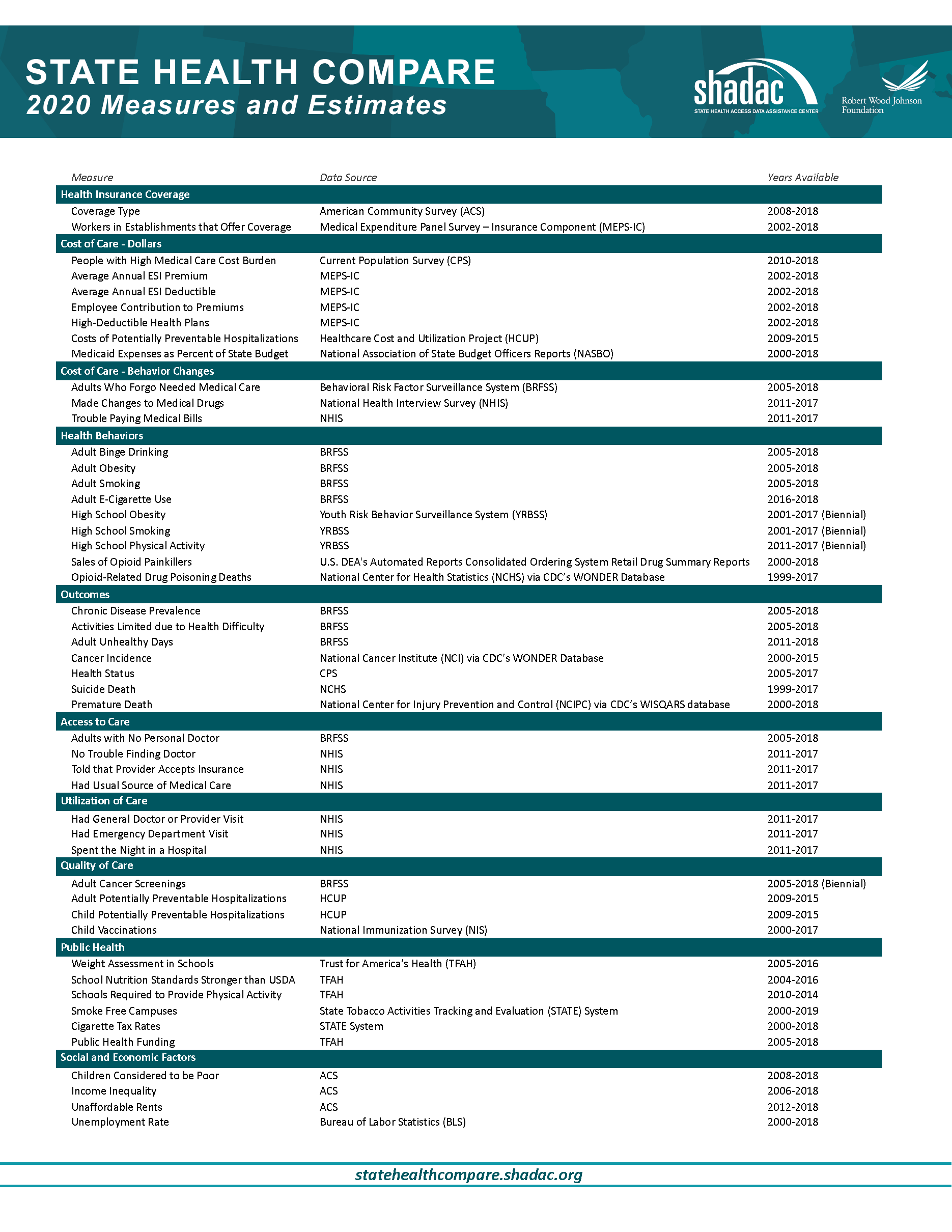
For a full overview of all available state-level measures, please visit the “Explore Data” page on State Health Compare, or take a look at our one-page guide to State Health Compare measures and their data sources.
All measures marked with an “*”: This indicates a break in series due to survey changes in either data processing or implementation methodology.
Blog & News
Internet Access Measures the Impact of the Digital Divide and COVID-19
March 27, 2020:The arrival of the novel coronavirus (COVID-19) has fundamentally changed the way we work, live, and seek health care. As more and more of the population across the United States is being asked to stay in their homes to assist the efforts toward containment and prevention of the virus, access to the internet has become a vital lifeline for families and individuals to keep in touch with their loved ones, participate in online school activities, and to work from home. Several sectors (business, government, health care, education, etc.) have embraced internet service-based solutions to keep connected. These activities have centered around:

These shifts not only test the capabilities of our current broadband internet systems, but also bring into sharp relief an issue commonly known as the “digital divide,” or the divide between individuals who have access to telecommunications and internet service (including the ability to connect to broadband in-home) and those who do not.2
SHADAC has added a new measure to our state data web tool, State Health Compare, to provide information about the digital divide at the state level and for key subpopulations: the percentage of households with access to broadband internet services. From an initial analysis of the newly available estimates, our findings show variation in access to broadband across states, and reveal disparities by income, rurality, coverage, and disability status.* We discuss these findings in more detail below.
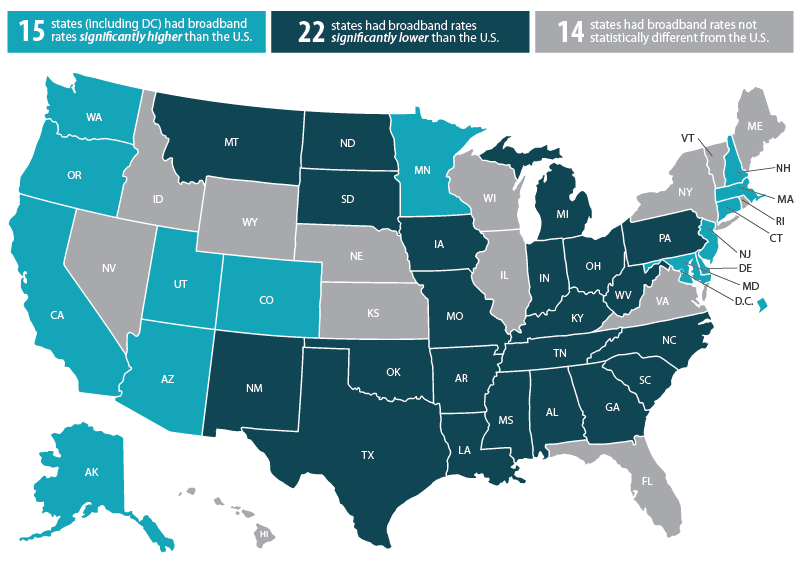
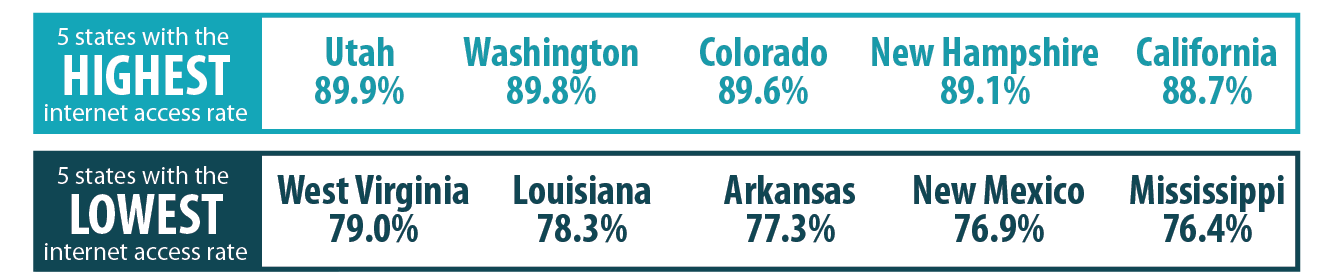
State Variation in Internet Access
Rates of broadband internet access ranged substantially across states in 2018, from a high of 89.9 percent in Utah to a low of 76.4 percent in Mississippi. When compared to the national rate (85.0 percent)...
Access to Broadband Internet Service by…
Household Income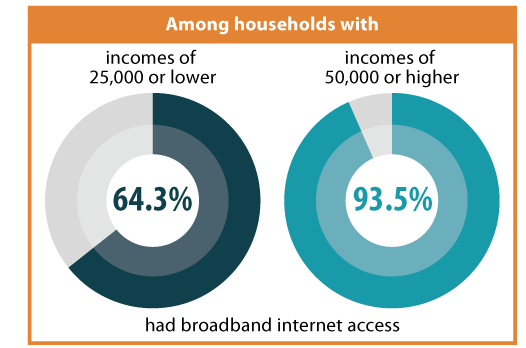
Nationally, households with incomes of $50,000 or higher were 45 percent more likely to have broadband internet access than households with incomes less than $25,000 (93.5 percent vs. 64.3 percent).
- In all 50 states and D.C., households with incomes $50,000 or higher were over 25 percent more likely to have broadband internet access than households with less than $25,000 in income.
- In 17 states, this disparity of access rose to 50 percent when comparing households with incomes $50,000 or higher to households with less than $25,000 in income.
Metropolitan Area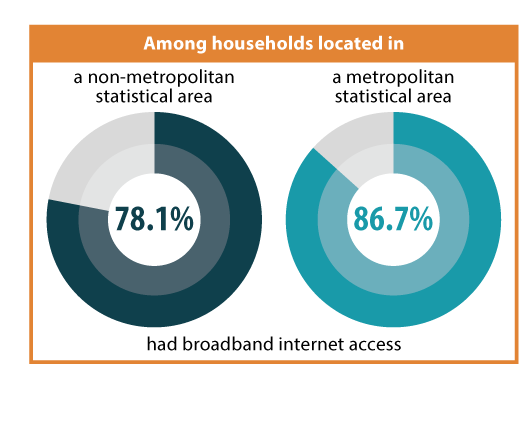
Nationally, households that were located in a metropolitan statistical area (MSA) were 11 percent more likely to have broadband internet access than households located in a non-metropolitan area (86.7 percent vs. 78.1 percent). Among the 44 states where estimates of broadband internet access by MSA/non-MSA were available:
- Households located in metropolitan areas had higher rates of broadband internet access than households in non-metropolitan areas in 39 states.
- In nine states (Alaska, Arizona, Arkansas, Florida, Georgia, Hawaii, Louisiana, Mississippi, Virginia), households located in metropolitan areas were over 20 percent more likely to have broadband internet access than their non-metropolitan counterparts.
- In Arizona, the disparity in access rose to over 60 percent when comparing metropolitan to non-metropolitan households.
Medicaid Coverage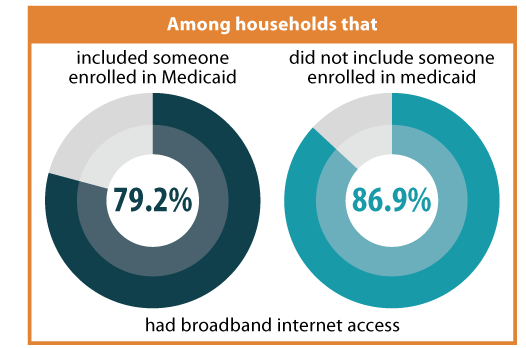
Nationally, households that included someone enrolled in Medicaid were approximately 9 percent less likely to have broadband internet access than households that did not include an individual with Medicaid coverage (79.2 percent vs. 86.9 percent).
- In 19 states (including DC), households that included someone with Medicaid coverage were over 10 percent less likely to have internet access than households that did not include a Medicaid enrollee.
- This gap in access more than doubled in D.C., where households that included someone with Medicaid coverage were over 20 percent less likely (21.4 percent) to have internet access than households not including a Medicaid enrollee.
Disability Status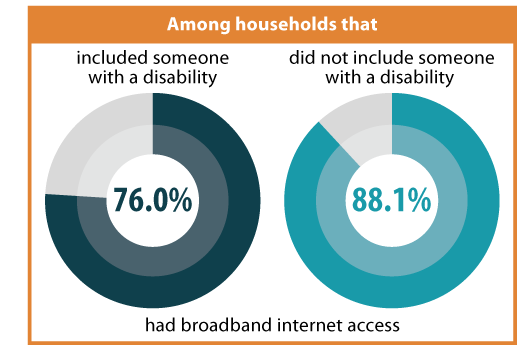
Nationally, households that included someone with a disability were approximately 14 percent less likely to have broadband internet access than households that did not include anyone with a disability (76.0 percent vs. 88.1 percent).
- In 23 states (including D.C.), households that included someone with a disability were over 15 percent less likely to have internet access than households that did include someone with a disability.
- In four states (Alabama, Maine, Minnesota, and Mississippi) and D.C., households that included someone with a disability were over 17 percent less likely to have internet access than households that did not.
Discussion
The lack of equitable access to broadband internet services across all households has been an issue of concern among health care experts even prior to the coronavirus pandemic. Initially, the problem of digital divide was studied in terms of barriers to health plan application and enrollment during the rollout of the newly developed online health insurance marketplace.3
Now, in light of recent events, lack of access to broadband internet services has also emerged as a potential challenge to efforts to respond to the coronavirus; not only in preventing individuals from accessing the real-time information they need surrounding COVID-19, but also in lost chances for utilization of telemedicine services, ability to work remotely, keeping pace with an e-learning curriculum, or to help mitigate the dangers of social isolation while practicing social distancing.4
Notes and Definitions
* All differences described in this blog are statistically significant at the 95% confidence level unless otherwise specified.
In the definition of the new State Health Compare measure, a broadband subscription includes a cellular data plan, cable, fiber optic, or DSL or satellite internet service. Households with a broadband subscription only include those who pay a cell phone or internet provider for the service. The percent of households that have access to broadband without paying for it is relatively small (approximately 3% in 2018).
Households' metropolitan status is determined at the public use microdata area (PUMA) level. Households are classified as “metropolitan” if their PUMA lies entirely inside a metropolitan statistical area (MSA) and are classified as “non-metropolitan” if their PUMA lies entirely outside an MSA.
“Medicaid enrollment” is defined as at least one person in the household having Medicaid coverage and “disability” is defined as at least one person of the household having a functional disability.
Related Resources
General Provider Telehealth and Telemedicine Tool Kit
The Coronavirus Outbreak Could Finally Make Telemedicine Mainstream in the U.S.
Opportunities to Expand Telehealth Use amid the Coronavirus Pandemic
Connectivity Considerations for Telehealth Programs
Telemedicine during COVID-19: Benefits, limitations, burdens, adaptation
Growth of Telemedicine Slowed by Internet Access Challenges
References
1 One of the most publicized and recognizable notices recently came from the Centers for Medicare & Medicaid Services, which expanded Medicare telehealth services. Centers for Medicare & Medicaid Services (CMS). (2020, March 17). Medicare telemedicine health care provider fact sheet. https://www.cms.gov/newsroom/fact-sheets/medicare-telemedicine-health-care-provider-fact-sheet
2 Congressional Research Service. (2020, March 13). COVID-19 and broadband: Potential implications for the digital divide. https://crsreports.congress.gov/product/pdf/IN/IN11239
3 Boudreaux, M.H., Gonzales, G., & Blewett, L.A. (2016). Residential high-speed internet among those likely to benefit from an online health insurance marketplace. INQUIRY, 53, 1-7. https://doi.org/10.1177/0046958015625231
4 Henning-Smith, C. (2020, March 18). COVID-19 poses an unequal risk of isolation and loneliness. The Hill. https://thehill.com/opinion/healthcare/488215-covid-19-poses-an-unequal-risk-of-isolation-and-loneliness
Publication
BRFSS Spotlight Series
|
BRFSS SPOTLIGHT SERIES OVERVIEW |
Estimates are from SHADAC analysis of the Behavioral Risk Factor Surveillance System and are available on State Health Compare.
Blog & News

BRFSS Spotlight Series: Adult Obesity Prevalence in the United States (Infographic)
March 17, 2020:|
BRFSS SPOTLIGHT SERIES OVERVIEW |
Click on the infographic image to enlarge
Adult Obesity
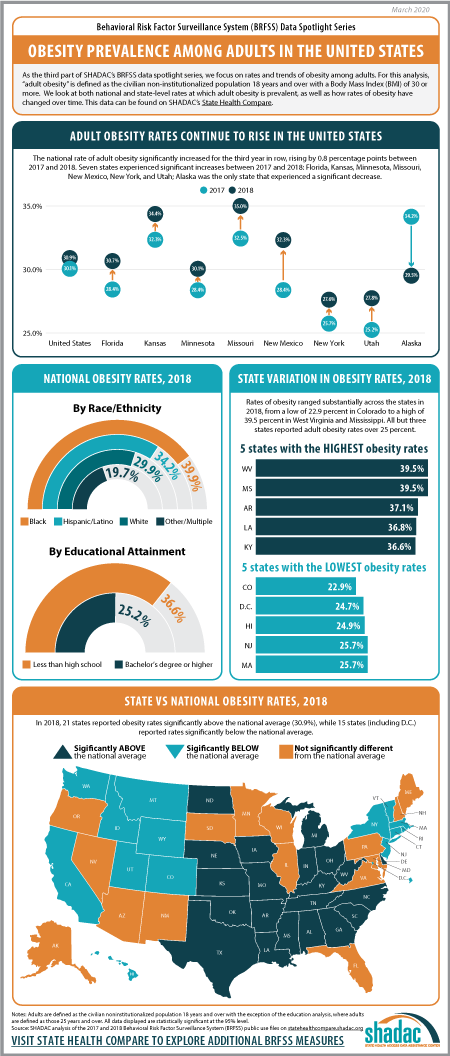
For the final post in our BRFSS Spotlight Series blog, we focused on trends in adult obesity rates. Though much attention has been paid to issues such as the opioid crisis or the rapid rise in youth vaping and e-cigarette use, the prevalence of obesity in the United States since the 1980s has made this one of the longest-running, currently declared public health emergencies in the nation.1
“Obesity” is defined as a Body Mass Index (BMI) of 30 and over, and the measure of “Adult Obesity” from the BRFSS encapsulates the self-reported prevalence of obesity among adults for the civilian non-institutionalized population 18 years and over. In using these BRFSS estimates, it is important to understand that self-reported data like these underestimates obesity rates as compared with the measured data from the National Health and Nutrition Examination Survey (NHANES). A 2016 research article from Ward et al. demonstrates a bias correction method for the BRFSS estimates that is beyond the scope of this analysis, but may be of interest to researchers.
Trends in Obesity Rates from 2017 to 2018*
The rate of adult obesity significantly increased for the third year in row nationwide from 2017 to 2018, rising by 0.8 percentage points to 30.9 percent from 30.1 percent in 2017.
Seven states experienced statistically significant increases in the rate of adult obesity from 2017 to 2018: Florida, Kansas, Minnesota, Missouri, New Mexico, New York, and Utah. Alaska was the only state to experience a statistically significant decline in the rate of obesity, decreasing 4.6 percentage points from 34.2 percent in 2017 to 29.5 percent in 2018.
Overall, however, a large majority of states (43 including D.C.) did not experience a statistically significant change in obesity rates from 2017.
State Variation (2018)
Rates of obesity ranged substantially across the states in 2018, from a high of 39.5% in West Virginia and Mississippi to a low of 22.9% in Colorado. When compared to the national rate…
- 21 states had obesity rates that were significantly higher.
- 15 states (including DC) had obesity rates that were significantly lower.
- 15 states had obesity rates that were not statistically different.
Persistently high rates of obesity are concerning in their own right, but also because obesity increases the risk for other serious health conditions such as heart disease, diabetes, stroke, and certain types of cancers, among many others.2
Unfortunately, current projections for the future indicate that the already high rates of obesity in America will only continue to increase. Without new interventions to prevent the spread of obesity, a new study using data from the BRFSS and published in the New England Journal of Medicine predicts that by 2030, nearly half of the United States population (48.9 percent) will be considered obese, with over a quarter of the nation registering as severely obese.
Notes
*All differences described here are significant at the 95% level of confidence unless otherwise specified.
For this analysis, adults are defined as those age 18 and over.
Estimates are from SHADAC analysis of the 2018 Behavioral Risk Factor Surveillance System and are available on State Health Compare.
1 Centers for Disease Control and Prevention (CDC). (1999, October 26). Obesity epidemic increases dramatically in the United States: CDCD director call for national prevention effort. Retrieved from https://www.cdc.gov/media/pressrel/r991026.htm
Health tidbits. (1999). J Natl Med Assoc, 91(12), 645. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2608606/
2 Centers for Disease Control and Prevention (CDC). (2020, February 4). Adult obesity causes & consequences. Retrieved from https://www.cdc.gov/obesity/adult/causes.html#Consequences
Blog & News
BRFSS Spotlight Series: Adult Binge Drinking Rates in the United States (Infographic)
February 27, 2020:|
BRFSS SPOTLIGHT SERIES OVERVIEW |
Click on the infographic image to enlarge
Adult Binge Drinking*
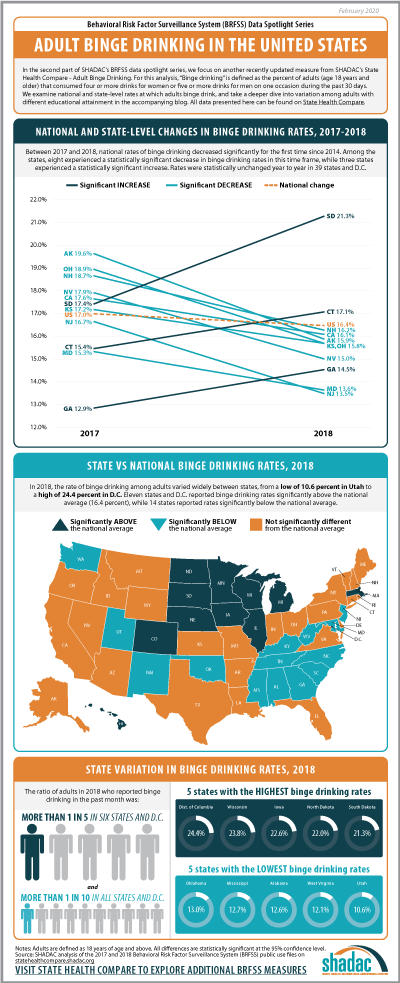
For this second post in our BRFSS Spotlight Series blog, we focus on an analysis of our Adult Binge Drinking measure (for which all differences described are statistically significant at a 95% confidence level unless otherwise specified). “Binge drinking” is defined by the Centers for Disease Control and Prevention (CDC) in the BRFSS as “drinking 5 or more drinks on an occasion for men or 4 or more drinks on an occasion for women" in the past 30 days.1
Over the past five years, adult binge drinking at the national level has increased a small but statistically significant amount from 16.0 percent in 2014 to 16.4 percent in 2018. For this analysis we also examined binge drinking by educational attainment, and found that adults (25 years and over) with a bachelor’s degree or higher in the U.S. reported a binge drinking rate of 15.7 percent in 2018, up from 15.3 percent in 2014 (percentage point difference was not statistically significant); and adults with less than a high school degree reported a rate of 13.5 percent in 2018, up from 12.8 percent in 2014.
Trends in Binge Drinking Rates from 2017 to 2018
Nationally, rates of binge drinking fell by 0.6 percentage points from 17.0 percent in 2017 to 16.4 percent in 2018—the first decrease since 2014. Statistically significant decreases in rates of binge drinking were seen in eight states: Alaska, California, Kansas, Maryland, New Hampshire, New Jersey, Nevada, and Ohio. Rates of binge drinking were statistically unchanged year to year in 39 states and D.C. Rates of binge drinking increased significantly in three states from 2017 to 2018: South Dakota, which experienced an increase of 3.9 percentage points (17.4 percent to 21.3 percent); Connecticut, which saw a 1.7 percentage-point increase (15.4 percent to 17.1 percent); and Georgia, with an increase of 1.6 percentage points (12.9 percent to 14.5 percent) between the two years.
State Variation (2018)
In 2018, rates of binge drinking varied widely between states, from a low of 10.6 percent in Utah to a high of 24.4 percent in D.C. Eleven states and D.C. reported rates of binge drinking above the national average (16.4 percent), and 14 states reported rates that fell below.
More than one in five adults reported binge drinking in the past month in six states—Iowa, Minnesota, Nebraska, North Dakota, South Dakota, and Wisconsin—and D.C., of which all but the latter were Midwest or Plains states.
Binge Drinking Rates across Education Levels+
Nationally, adults with less than a high school education were 14.1 percent less likely to report binge drinking compared to adults with a bachelor’s degree or higher level of education (13.5 percent vs. 15.7 percent).
Among the 48 states and D.C. where estimates of binge drinking among adults with a less than a high school education were statistically reliable^:
- Utah was both the only state where adults with less than a high school education were statistically more likely to report binge drinking than adults with a bachelor’s degree or higher, and also the state with the largest relative gap (89.2 percent) in binge drinking rates by education (14.7 percent vs. 7.8 percent).
- Adults with less than a high school education were statistically less likely to report binge drinking compared to adults with a bachelor’s degree or higher in 14 states, and the size of this gap varied from a low of 19.4 percent in Minnesota (15.1 percent vs. 18.8 percent) to a high of 56.6 percent in Missouri (7.8 percent vs. 17.9 percent).
- There was no statistically significant difference between these groups’ rates of binge drinking in 33 states and D.C.
This analysis follows recent trends reported by the Centers for Disease Control and Prevention, which indicates binge drinking is more common among people of higher educational levels and with household incomes of $75,000 or more. Individuals with lower incomes and educational levels in the U.S., however, consume more binge drinks (i.e., number of drinks in a binge drinking occasion) per year.2
Notes
All differences described in the post are statistically significant at the 95% confidence level unless otherwise specified.
* Rate of binge drinking among adults for the civilian noninstitutionalized population 18 years and over.
+ For the education analysis, adults are defined as those age 25 and older.
^ Estimates were considered statistically unreliable if the standard error was more than 30% as large as the estimate (i.e., RSE > 30%) - in this instance, estimates were statistically unreliable for Alaska and New Jersey.
References
1Centers for Disease Control and Prevention (CDC). (2020, January 2). Data on excessive drinking. Retrieved from https://www.cdc.gov/alcohol/data-stats.htm.
There is some differentiation between agencies (such as the CDC, National Institute of Alcohol Abuse and Alcoholism [NIAAA], and the National Institute of Health [NIH]) over whether binge drinking is defined as four drinks for women and five drinks for men on “one occasion” or “within a two-hour period,” but the question included in the BRFSS uses the “on one occasion” phrasing.
2 Kanny D, Naimi TS, Liu Y, Lu H, Brewer RD. (2018). Annual total binge drinks consumed by U.S. adults, 2015. Am J Prev Med, 54(4), 486-496.

