On July 30th, 1965, President Lyndon B. Johnson signed the legislation that established the Medicaid program into law, providing millions of Americans with health care coverage.
But what is Medicaid, exactly? Who is eligible for Medicaid? How is Medicaid funded? And why does Medicaid vary from state to state?
In honor of Medicaid’s 60th anniversary, the following blog aims to answer each of these questions, as we walk our readers through the origins of the Medicaid program, how Medicaid is funded, and how its flexibility supports innovation and tailored programs for each state’s unique population.
What Is Medicaid? Medicaid Origins, Financing, and Stats
Let’s start with the basics of the program, including what it is, when it was established, who it serves, and how it functions.
What Is Medicaid?
Medicaid is a joint federal-state program that provides health insurance coverage to eligible individuals. While both federal and state governments contribute financially to Medicaid (more on this later), Medicaid programs are administered by each individual state; all 50 states, the District of Columbia, and all five U.S. territories have their own Medicaid programs.*
One reason Medicaid varies from state to state is that while federal guidelines establish minimum requirements that the programs must follow, states have flexibility to tailor eligibility criteria, covered services, and delivery models to meet the needs of their unique populations and communities. We’ll cover more on Medicaid at the state level in a following section.
To learn more details about the basics of Medicaid, check out this playlist of Medicaid 101 videos from the Medicaid and CHIP Payment Access Commission (MACPAC).
When Was Medicaid Established?
Medicaid was first established in July 1965 with the signing of the Social Security Amendments of 1965 into law, which later came to be known as the Medicare and Medicaid Act. See figure below for a general timeline of the Medicaid program.
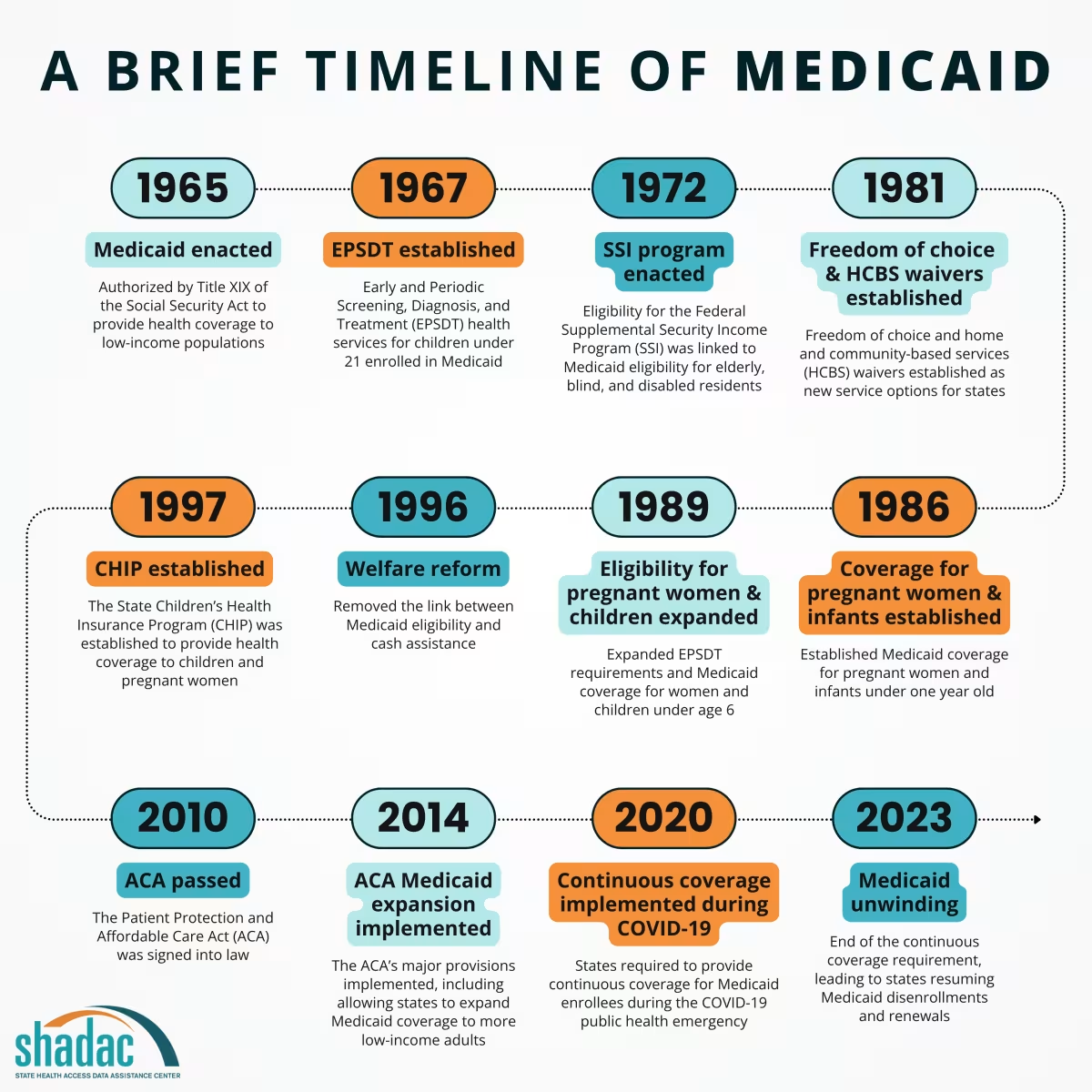
At the time, policymakers were focused on providing coverage for the “aged” population through Medicare, as evidenced in the subheadings of the original document. However, one line also mentioned the establishment of a program for "individuals receiving money payments under public assistance programs.” This insertion was the official establishment of the Medicaid program, and its haphazard inclusion underscored its secondary importance to the Medicare program in the eyes of policymakers and the nation at the time of its founding. This also serves as the basis for the long-held perception of Medicaid as a program for “low-income individuals.”
Medicaid vs Medicare: What’s the Difference?
While similar in name and sharing similar goals of providing coverage to those in need, Medicaid and Medicare programs are distinct in whom they cover and how they are financed.
Medicaid is funded by both the federal government and state governments and is administered by individual states. Just as the programs vary by state in their coverage of distinct services and benefits, so do Medicaid eligibility guidelines. However, Medicaid mainly aims to serve certain populations of adults and children under 65—historically, those with limited or low incomes, those with disabilities, and those who are pregnant.
Medicare, on the other hand, is a solely federal health insurance program that provides coverage to people 65 and older (and some under 65 with certain disabilities/conditions). Because this is a federal program, Medicare coverage is the same regardless of which state a person lives in.
How Is Medicaid Federally Funded?
Medicaid funding is unique in that it is shared by both the federal government and state governments. As we detail in this blog on Medicaid as a countercyclical policy:
“States take on a majority of the responsibilities for the design and implementation of their Medicaid programs compared to the federal government [...] with the federal government generally paying a larger share of Medicaid costs [...] The precise amount of federal funding that states receive for their Medicaid programs varies based on a variety of factors determined by federal law.”
The actual percentage of Medicaid costs covered by the federal government is known as the “federal medical assistance percentage,” or “FMAP.” Generally, a state’s FMAP varies based on income compared to the national average with “the federal government pay[ing] a higher share of Medicaid spending for lower-income states than it does for higher-income states.”1 In fiscal year 2025, FMAP levels range from a minimum of 50% to a maximum of 83%.
To learn more, you can find FMAPs by state for 2022–2025 in MACPAC’s MACStats: Medicaid and CHIP Data Book.
60 Years of Medicaid: Current Medicaid Stats
Today, 60 years after it was established, Medicaid covers 1 in 5 Americans, including 40% of all children and 60% of all nursing home residents.2 Preliminary data from March 2025 estimates that 71.3 million people were enrolled in Medicaid.3
Over the years, the Medicaid program has evolved, expanding and adjusting eligibility, services, and programs. For example, when the Affordable Care Act (ACA) was implemented in 2013, it allowed states to choose whether to expand their Medicaid programs to offer coverage to all adults with incomes below a certain level. As of this writing, 40 states and Washington, D.C. have adopted Medicaid expansion via the ACA.
We can also see that Medicaid is a key source of coverage for specific populations, and a top payer for key services:
- More than 8 in 10 children who live in poverty are covered by Medicaid4
- One-third (33.9%) of Medicaid enrollees self-identify as having a disability (roughly double the overall national rate of 16.9%)5
- An estimated 27.6% of Medicaid enrollees age 18-64 report having a mental illness6
- Medicaid is the largest payer of behavioral health services in the U.S., including mental health and substance use services7
- 40% of all births, and almost 50% of births in rural areas, are covered by Medicaid8
- Medicaid is the top payer of long-term services and supports (LTSS) in the country9
Medicaid-Eligible Populations
Let’s look a bit closer at the details of the populations and communities eligible for Medicaid.
Who Is Eligible for Medicaid?
In the years since Medicaid’s founding, coverage has expanded dramatically such that: 1) Medicaid has overtaken Medicare in number of enrollees (71.3 million vs 68.6 million individuals);10 and 2) a number of different population groups beyond “low-income individuals” are now eligible for Medicaid, including:
- Children younger than 19 whose family’s or guardian’s income does not exceed 133% FPL; newborns of women covered by Medicaid; children with disabilities; children who use long-term services and supports due to a medical condition or disability; and some children in foster care or adoption assistance programs.
- Adults with physical, intellectual, or developmental disabilities; pregnant women with incomes less than 133% FPL; low-income parents or other caretakers with dependent children (such as foster care adults); adults over 65 with low-incomes and in need of nursing home or long-term care services not covered by Medicare (also referred to as “dual-eligibles”).11
Additionally, with the establishment of the ACA, states were given an option to expand Medicaid coverage eligibility to non-disabled adults whose income is up to 138% FPL, or about $21,000 per year for one person. One of the most important impacts of Medicaid expansion is that it has increased the number of people with health insurance coverage by more than 38 million and nearly halved the nation’s uninsured rate (falling from 14.4% in 2013 to 7.9% in 2023).12
Through various coverage expansions, Medicaid now serves a larger and more diverse population of eligible enrollees. A recent study of coverage between 2008 (pre-ACA) and 2023 (post-Medicaid unwinding) found that Medicaid expansion increased enrollment among children, Asian Americans, Black Americans, and individuals living in urban areas the most, though enrollment increased among all resident groups in expansion states. By 2023, 18.6 million new adults were enrolled in Medicaid through eligibility pathways created by the ACA expansion.
Medicaid at the State Level
50 State-Administered Medicaid Programs, Many Unique Names
With each of the 50 states and the District of Columbia running their own Medicaid programs, many also have their own unique name, which you can find listed in our State Health Insurance Program Names resource. The design, administration, and implementation of Medicaid is also unique to each state.
Why Does Medicaid Vary from State to State?
As briefly discussed above, both the federal government and state governments contribute financially to their distinct programs. However, individual states administer their own Medicaid programs, allowing for flexibility in how the programs operate. Eligibility and benefits also differ by state.
How Is Medicaid Funded by States?
The Medicaid program is both a significant expenditure for states and a source of federal funding. Although the federal government provides considerable funding for the program, states also commit substantial financial resources. As we explored in this short brief, states use a multitude of mechanisms to fund Medicaid, such as state and local taxes, fees and assessments, general funds or other specialized funds, among others.
Medicaid accounts for a major share of state budgets, often registering as the second-largest category behind K-12 education funding. Data from State Health Compare shows that in 2023 (the most recent data year available), the percent of state budgets spent on Medicaid ranged from a low of 13.4% in Wyoming to a high of 41.6% in Texas.
How Is Medicaid Administered by States?
While the Centers for Medicare and Medicaid Services (CMS) serves as the federal governing body for Medicaid, each individual state has their own agency to administer the program. Depending on the state, Medicaid can be housed as a standalone agency or underneath the umbrella of the state’s Department of Health or Department of Health and Human Services.
Each state also has a Medicaid Director (a list of Medicaid Directors can be found here). While the specifics can change from state to state due to the unique makeup of the program, Medicaid Directors serve as the bridge between the federal and state partnership in running the program and are generally in charge of overseeing the functionality of Medicaid services offered in the state.13
More recently, a new federal rule requires every state to establish a Medicaid Advisory Committee (MAC) to advise the state’s Medicaid agency, ensure proper program administration, and certify the program is working in the best interest of enrollees.
Each state also has a Beneficiary Advisory Council (BAC) composed of Medicaid beneficiaries, their families, and/or their caregivers. BAC members advise the state on a variety of matters, ranging from their lived experiences with the Medicaid program to potential new policy development to day-to-day specifics on administration of the program.
How Does Medicaid Coverage Vary Across States?
As there is variation across states in Medicaid spending and governance, there is also variability in who is covered from one state to another.
To better understand the variability, we looked at State Health Compare’s ‘Health Insurance Coverage Type’ measure. This measure displays the percentage of individuals in each state that fall under each health insurance type (e.g., Medicaid, private coverage, uninsurance, etc.).
In 2023, the state with the highest percentage of their population covered by Medicaid was New Mexico, with 25.6% enrolled in Medicaid. Utah was the state with the lowest percentage of their population covered by Medicaid, with only 7.9% being covered. In the interactive figure below, you can explore Medicaid/CHIP coverage rates across the states from 2008 to 2023.
There are some Medicaid benefits that programs in all 50 states are required by federal law to cover, including inpatient and outpatient hospital services, transportation to medical care, nursing facility services, and home health services. However, states can customize other service offerings within their programs such that they can provide additional benefits for the unique needs of their enrollees, such as dental services, physical therapy, prescription drugs, and other health services.
State-Level Innovations via Medicaid
As we have reviewed, centering the operations of Medicaid at the state level provides key flexibilities for states to innovate and tailor policies or practices, within federal guidelines, to meet the specific needs of a state and its residents.
In our over 20 years of experience in the field of health policy and public health, SHADAC has identified and worked with several states across the country eager to test new approaches to administering their Medicaid programs to improve program access, operations, and experiences.
Recently, SHADAC participated in a University of Minnesota research team tasked with supporting the state of Minnesota’s Equitable Health Care Task Force.
Part of this effort included scanning for equity-based policies and practices (and evidence of what works) in various topic areas, including value-based payment models and integration of health care and public health, amongst others, to inform the Task Force’s work. Notably, many of the case examples we found and included in the resource guide we developed for the Task Force came from state Medicaid agencies, highlighting their capacity for adaptability and innovation in serving beneficiaries.
In this section, we will review two promising areas of state-level innovation in Medicaid programs, highlighting some specific examples:
- Value-based payment models
- Coordination across medical and community-based services
Value-Based Payment Models
Over the last 15 years (since the passage of the ACA), a number of states have explored opportunities to address the rising costs of health care. Several states were already experimenting with delivery system and payment reform prior to the ACA, but the ACA’s passage accelerated that work.
State Medicaid agencies have continually sought ways to transform health care payment systems in order to incentivize improvement in patient health outcomes and well-being (value-based payment) as opposed to reimbursement based on the volume of services delivered.
One example of such state-level innovation is the State Innovation Models (SIM) initiative supported by the Center for Medicare and Medicaid Innovation (CMMI) and implemented between 2013 and 2020. This program allowed states to test and implement new strategies or payment models aimed at improving quality of care, lowering care costs, and improving the state population’s overall health. Although it was a multi-payer effort (inclusive of public and private insurance payers), most participating states relied heavily on their state Medicaid programs to design, implement, or monitor delivery system and payment reforms.
Even though the effects of 17 SIM Model Test states in terms of reduced costs and improved quality were mixed, many SIM test states have continued to sustain or even expand SIM programming, evolving and adjusting as needed. For example, the Minnesota Department of Human Services’ Medicaid Accountable Care Organization shared savings program, known as Integrated Health Partnership (IHP), has grown and evolved since its participation in SIM to reflect state priorities and beneficiary needs. (See SHADAC’s recent ‘Integrated Health Partnership’ blog for more on this innovative approach.)
Another example is TennCare, which continues to maintain and grow its ‘episodes of care’ program (see box).
| BOX: Tennessee Episodes of Care Program: Savings Achieved; Quality Maintained or Improved |
|---|
State - Tennessee Innovation - Clinical episode-based payment model Timeframe - 2013 design; 2014 - Present implementation Description - As part of an effort to move away from volume-based to value-based payment, Tennessee’s Medicaid agency known as Division of TennCare implemented a payment reform centered around episodes of care. This strategy was one of many the State implemented under the SIM initiative. An episode of care is all of the relevant health care services a patient receives during a specific time period to treat a specific condition. Episode-based payment incentivizes the provider (either a facility or an individual) who has the most impact over the overall cost and quality of a patient’s treatment through risk-sharing or gain-sharing payments. Rewards or penalties are calculated retrospectively according to spending targets and quality metrics. The State implemented its episodes of care program in waves; the first wave included its perinatal, asthma, and total joint replacement episodes. Currently 48 episodes of care are operated and maintained. TennCare Medicaid Managed Care Organizations prepare episode reports for participating providers. Population - Select Medicaid beneficiaries and commercially insured patients in the State. Goals/Effects - As of 2023, TennCare reports an estimate of $56.5 million in savings form its episodes of care program since 2015. About one third of providers received gain-sharing incentive payments, while only 8 percent made risk-sharing payments. The top five episodes of care with the highest volume of valid episodes were respiratory infection, otitis media, skin and soft tissue infection, back/neck pain, and UTI-outpatient. The top five episodes of care for which the State estimates the most savings were perinatal, UTI-outpatient, asthma, otitis media, and tonsillectomy. In 2023, quality metrics held steady or improved for most episodes. |
Box Source - 2023 Results and FAQs
Coordination Across Medical and Community-Based Services
State Medicaid agencies are also demonstrating innovative practices in terms of how they facilitate greater coordination across medical and community-based resources to address health and health-related social needs. These programs have led the way in promoting screening and referral for unmet needs, such as lack of healthy food, affordable housing, and access to transportation, as well as piloting community-based care coordination models.
One great example of this work is Medicaid programs’ use of Section 1115 demonstration waivers, which are named for their purpose of waiving certain requirements and allowing more innovative practice and policy testing to be implemented. Another related example is provisions in Medicaid managed care contracts to reimburse for, and improve access to, non-traditional Medicaid services.
Let’s look at these innovations in action. North Carolina, for example, implemented its Health Opportunities Pilots in 2022 under section 1115 waiver authority. The pilot relies on a standardized screening tool and networks of community-based referral organizations to provide needed non-medical services. Early evaluation findings suggest increased screening and decreased health-related social needs among participants.
Recently, the National Association of Medicaid Directors (NAMD) highlighted efforts in several other states that were granted federal waivers or amendments to collaborate with rural providers or community-based organizations to sustain access and improve health and well-being. Tested interventions ranged from addressing social determinants of health and related data exchange to mobile services and transportation supports.
And, a relatively new initiative out of Acumen American called Medicaid Innovation Collaborative “convenes states, health plans, and entrepreneurs to pilot technology solutions that address beneficiary social needs related to food security, housing affordability and quality, and transportation security.”
As states continue to evolve their programs to respond to current events and issues, SHADAC plans to monitor program progress and new efforts such as these. Each of these innovations is focused around a common goal to better serve the needs of the state’s residents covered by Medicaid.
The Impact of Medicaid Goes Beyond Enrollees
As this blog has covered, there are many individuals across the U.S. who are served by and benefit from the Medicaid program. Though it began quietly in the shadow of Medicare, Medicaid has now surpassed Medicare to become the largest singular source of health coverage in the U.S.** The unique structure, administration, and funding makeup of Medicaid as a partnership between states and the federal government allows for many flexibilities aimed at better serving beneficiaries.
The positive effects of Medicaid can also spread far beyond the individual directly receiving coverage. For instance, when Medicaid expansion was established via the ACA, several studies found that this had a “welcome-mat” effect on insurance coverage, “where individuals who were previously eligible for Medicaid had not signed up for coverage until after the ACA, potentially owing to greater awareness or ease of application.”14 Coverage expansion also provides greater financial stability for individuals and families, as Medicaid expansion has been found to decrease levels of out-of-pocket spending and other financial burdens due to medical care.
Medicaid coverage, flexibility, and innovation in payment systems aimed at better serving individuals can also have ripple effects outward that positively impact the entirety of the health care system. More directly, reimbursements from Medicaid to providers, even though they are lower than for private coverage, reduce the amount of uncompensated care costs for hospitals and clinics, offering greater financial security and enabling providers to keep the doors open to treat other patients. This can have an outsized effect on access to care for rural communities, where clinics and hospitals are fewer in number and patients must travel longer distances to get needed care.
Federal matching funds provided by Medicaid expansion have also provided financial stability for both states and providers. For the former, matching funds have allowed states to sustain programs that treat individuals with mental health issues and substance use disorders, and provide support for families. For the latter, expansion funding offset fiscal stress borne by providers treating certain populations, such as those likely to be uninsured, or those with more severe diagnoses, such as cancer and traumatic injuries.15
More indirectly, Medicaid can be a substantial driver of state and local economies: creating jobs for those in the health care sector, ensuring job stability for those able to seek care and remain healthy enough to continue working, and generating tax revenue for states.16
While the positive ripple effects of Medicaid’s establishment and subsequent expansion are too numerous to cover all in one blog,*** we hope that the examples shared here have provided readers with a better understanding of how Medicaid has expanded from its humble origins 60 year ago to become an essential source of health insurance coverage that so many individuals and families, and even providers, rely on today.
Notes
* The structure and coverage provided by Medicaid programs established in each of the five U.S. territories—Puerto Rico, the Virgin Islands, American Samoa, Guam, and the Northern Mariana Islands—differ so significantly from those established in the 50 states and D.C. that they are not discussed in this blog.
**The largest type of coverage in the U.S. is employer-sponsored insurance (covering 53.7% of the nation’s population). However, this category is comprised of a number of different insurers/payers, rather than a single overarching program/payer.
*** Researchers at the Kaiser Family Foundation (KFF) have attempted to create a comprehensive review of the effects of Medicaid Expansion under the ACA, with a series of reports reviewing evidence found in published studies that were released by KFF in 2020, 2021, and 2023.
Sources
[1] Worrall, C. (2025, June 24). What Is a “Countercyclical” Policy or Program? How Medicaid Protects People When the Economy Falters. State Health Access Data Assistance Center (SHADAC) Blog. https://www.shadac.org/news/countercyclical-fiscal-policy-program-medicaid
[2] American Hospital Association (AHA). (2025). Fact Sheet: Medicaid. https://www.aha.org/fact-sheets/2025-02-07-fact-sheet-medicaid
[3] Centers for Medicare & Medicaid Services (CMS). (2025). March 2025 Medicaid & CHIP Enrollment Data Highlights. Medicaid.gov. https://www.medicaid.gov/medicaid/program-information/medicaid-and-chip-enrollment-data/report-highlights.
[4] Kaiser Family Foundation (KFF). (2024, January 16). More Children are Losing Medicaid Coverage as Child Poverty Grows. https://www.kff.org/medicaid/press-release/more-children-are-losing-medicaid-coverage-as-child-poverty-grows/
[5] Zylla, E., & Lukanen, E. (2025, June 20). The Disability Gap in Medicaid: Implications for the Federal Work Requirement Proposal. State Health & Value Strategies (SHVS) Expert Perspectives. https://shvs.org/the-disability-gap-in-medicaid-implications-for-the-federal-work-requirement-proposal/
[6] Medicaid and CHIP Payment and Access Commission (MACPAC). (2021). Chapter 2: Access to Mental Health Services for Adults Covered by Medicaid. Report to Congress on Medicaid and CHIP. https://www.macpac.gov/wp-content/uploads/2021/06/Chapter-2-Access-to-Mental-Health-Services-for-Adults-Covered-by-Medicaid.pdf
[7] Georgetown Center for Children and Families (CCF). (2025). How Medicaid Helps People with Substance Use Disorders. Georgetown University McCourt School of Public Policy. https://ccf.georgetown.edu/2025/02/19/how-medicaid-helps-people-with-substance-use-disorders/
[8] American Hospital Association (AHA). (2025). Fact Sheet: Medicaid. https://www.aha.org/fact-sheets/2025-02-07-fact-sheet-medicaid
[9] Congressional Research Service (CRS). (2023, September 19). Who Pays for Long-Term Services and Supports? Library of Congress (Congress.gov). https://www.congress.gov/crs-product/IF10343
[10] Centers for Medicare & Medicaid Services (CMS). (2025). Medicare Monthly Enrollment. https://data.cms.gov/summary-statistics-on-beneficiary-enrollment/medicare-and-medicaid-reports/medicare-monthly-enrollment
[11] National Center for Health Statistics (NCHS). (2025, June 9). Medicaid. Health in the United States. https://www.cdc.gov/nchs/hus/sources-definitions/medicaid.htm
[12] Hest, R. (2025, March 24). 15 Years of the Affordable Care Act: More Americans Than Ever Have Health Insurance Coverage. State Health Access Data Assistance Center (SHADAC) Blog. https://www.shadac.org/news/15-years-affordable-care-act-more-americans-ever-have-health-insurance-coverage
[13] National Association of Medicaid Directors (NAMD). (n.d.) NAMD’s 1st Annual Medicaid Operations Survey: Summary. https://medicaiddirectors.org/wp-content/uploads/2012/06/namd_mcdops_summary_final_102612.pdf
[14] Kominski, G.F., Nonzee, N.J., & Sorenson, A. (2018, April 5). The Affordable Care Act’s Impacts on Access to Insurance and Health Care for Low-Income Populations. Annual Review of Public Health, 38, 489-505. 10.1146/annurev-publhealth-031816-044555
[15] Guth, M. & Ammula, M. (2023, January 18). What Does the Recent Literature Say About Medicaid Expansion?: Economic Impacts on Providers. Kaiser Family Foundation (KFF). https://www.kff.org/medicaid/issue-brief/what-does-the-recent-literature-say-about-medicaid-expansion-economic-impacts-on-providers/
[16] Horstman, C., Federman, S., Richards, C., & Coleman, A. (2025, May 5). How Does Medicaid Benefit States? Commonwealth Fund. https://www.commonwealthfund.org/publications/explainer/2025/may/how-does-medicaid-benefit-states